At Modal Pain Management in NYC, Dr. Alex Movshis specializes in epidural steroid injections as part of our comprehensive, non-surgical approach to pain management. Epidural steroid injections are among the most commonly performed and highly effective interventional procedures for treating radicular pain — a pinched nerve — along with sciatica, herniated discs, and chronic lower-back and neck pain. Rather than relying solely on medications that merely mask symptoms, these targeted injections deliver anti-inflammatory medication directly to the source of pain—the epidural space surrounding your spinal cord and nerve roots. This precise approach allows many of our patients to avoid surgery, resume their daily activities, and achieve meaningful pain relief in a matter of days to weeks.
How Epidural Steroid Injections Work
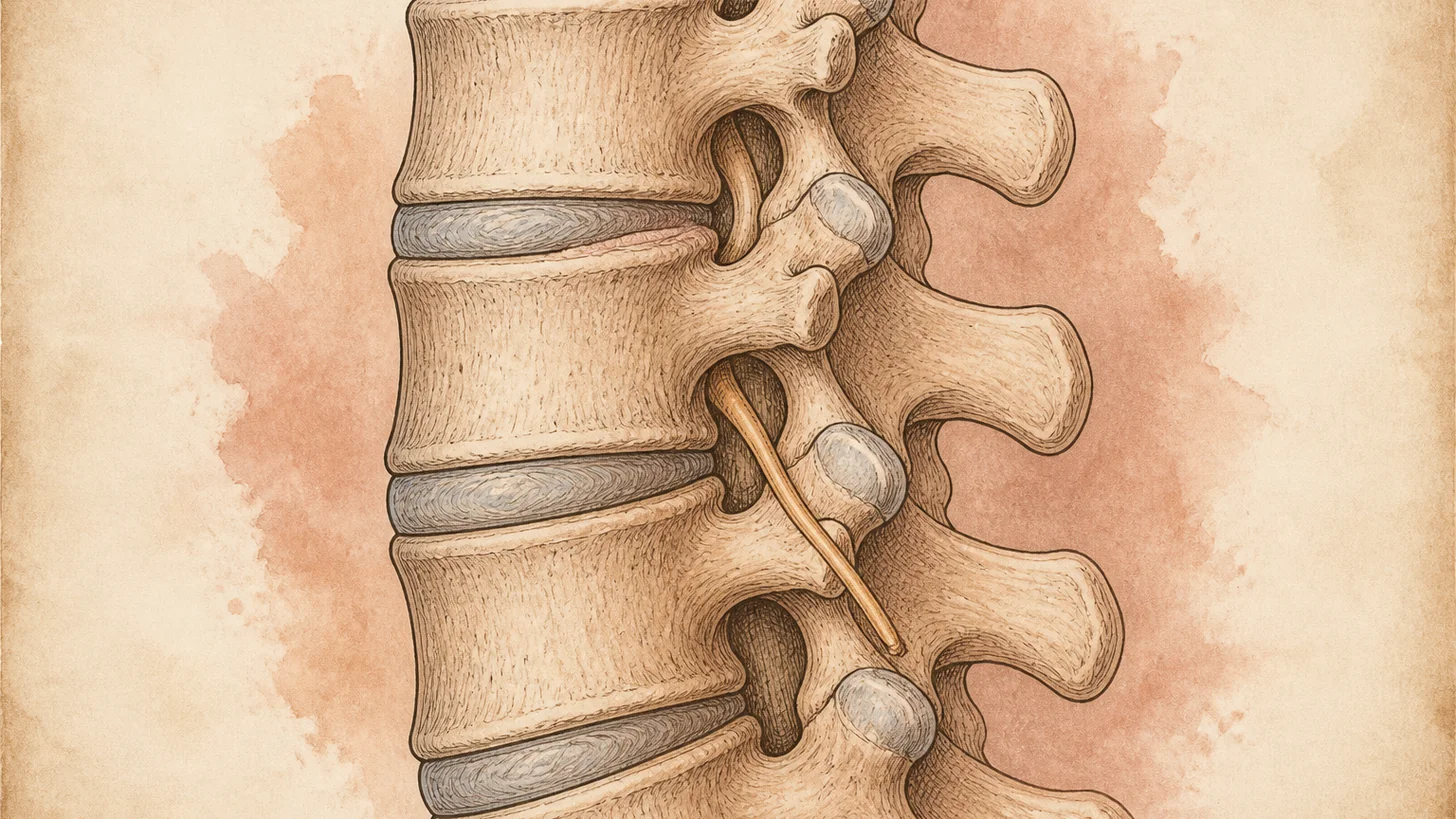
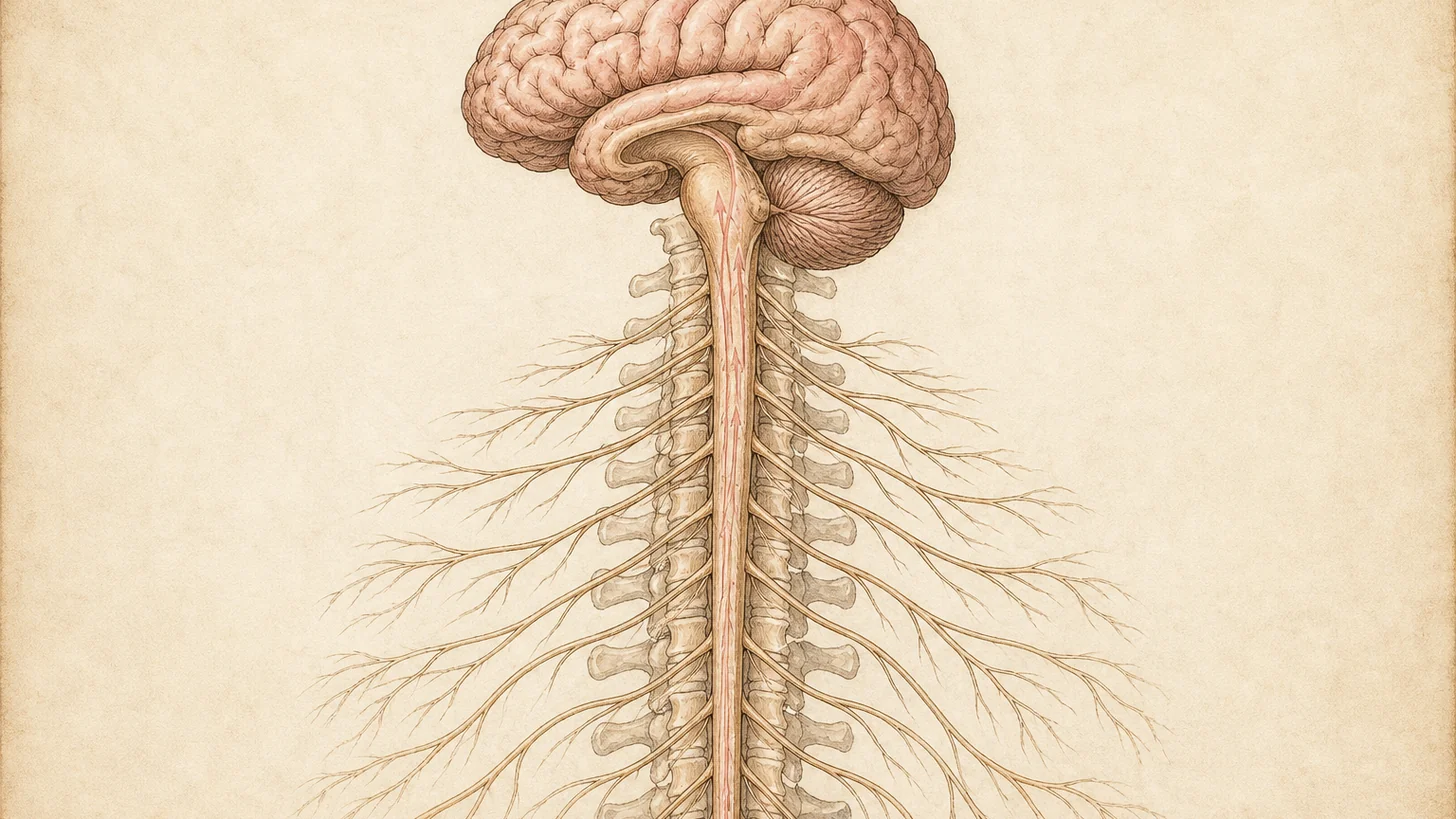
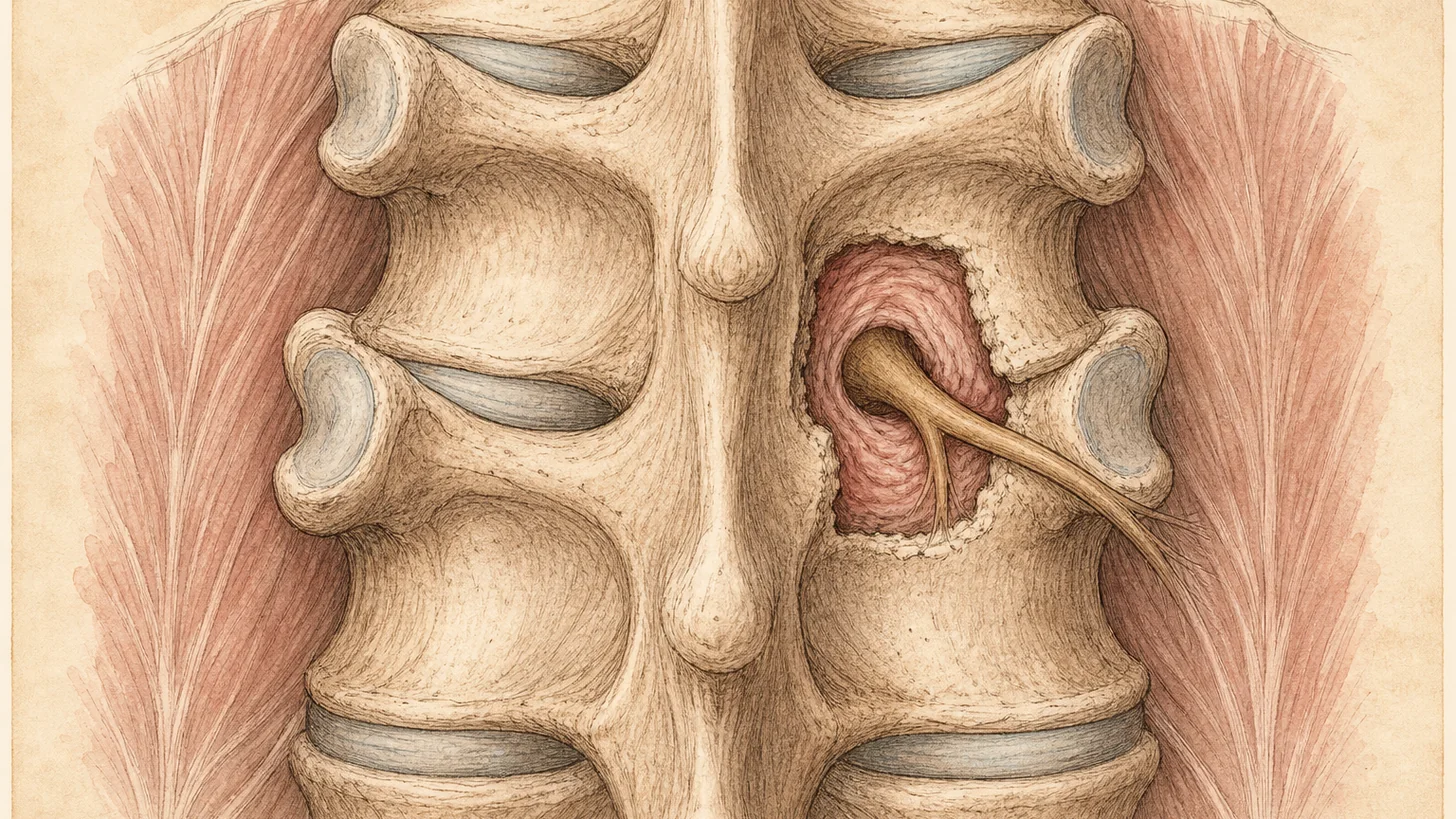
The epidural space is the area between the dura mater (the outermost membrane protecting the spinal cord) and the vertebral bone. When spinal structures become inflamed due to herniated discs, degenerative changes, or other conditions, they can irritate nearby nerve roots, causing pain that radiates into your legs, arms, or buttocks. During an epidural steroid injection, Dr. Movshis uses advanced fluoroscopic X-ray guidance to visualize the spine in real time, ensuring the needle reaches the exact location where inflammation is occurring. This fluoroscopic precision is crucial for safety and effectiveness, allowing the steroid medication and local anesthetic to be deposited exactly where they’re needed. The steroid reduces inflammation around the affected nerve root, while the anesthetic provides immediate pain relief. The combination addresses both the short-term pain and the underlying inflammatory process causing your symptoms.
Conditions We Treat with ESIs
Epidural steroid injections effectively treat multiple spinal conditions that cause radicular pain. Herniated discs are among the most common indications—when the inner nucleus of a disc bulges outward, it can compress and inflame nearby nerve roots, causing shooting pain. Lumbar spinal stenosis, a narrowing of the spinal canal often due to age-related degenerative changes, compresses multiple nerve roots and responds well to ESI therapy. Sciatica, characterized by pain radiating from the lower back through the buttocks and leg, often results from disc herniation or foraminal stenosis and typically improves significantly with these injections. Degenerative disc disease, where discs lose height and hydration over time, frequently causes inflammation that responds to steroid medication. Additionally, ESIs help patients with radiculopathy from various causes, facet-mediated referred pain, and post-surgical scar tissue inflammation.
Types of Epidural Injections
Dr. Movshis selects the approach that best targets your specific pathology. Interlaminar injections pass the needle between adjacent vertebral laminae to reach the epidural space, providing broad coverage and working well for central canal stenosis or bilateral symptoms. Transforaminal injections are directed toward the neural foramen where the nerve root exits the spine, offering the most direct access to the affected nerve and preferred for lateral disc herniations or foraminal stenosis. Caudal injections are performed at the base of the spine and are excellent for treating lower lumbar and sacral pain, particularly in patients where other approaches are anatomically difficult. Each approach is selected based on your imaging findings, symptom distribution, and anatomy to maximize the likelihood of relief.
Effectiveness and Benefits
Epidural steroid injections provide relief for 50-90% of patients with radicular pain or sciatica, with some studies showing even higher success rates when combined with physical therapy. Many patients experience relief within 24-48 hours, though maximum benefit typically develops over 1-2 weeks as inflammation decreases. Unlike oral pain medications that affect your entire body and carry risks of dependence or gastrointestinal side effects, these injections target inflammation at its source. This targeted approach means faster pain relief without systemic effects, allowing you to engage in rehabilitation and return to activities more quickly.
What to Expect During the Procedure
Your epidural steroid injection procedure takes approximately 15-20 minutes in our office-based setting. You’ll be positioned on the procedure table—either prone (lying face-down) or on your side, depending on which approach Dr. Movshis recommends. The skin is cleaned with sterile antiseptic solution, and a local anesthetic numbs the area. You may feel pressure as Dr. Movshis advances the needle, but the local anesthetic ensures the procedure is not painful. Real-time fluoroscopic guidance allows precise needle placement. Once positioned correctly, the steroid and anesthetic medication are gently injected. You’ll typically rest for 15-20 minutes afterward before going home. Most patients can return to light activities immediately, though strenuous activity should be avoided for 24-48 hours.
Treatment Course and Maintenance
Most patients receive a series of 2-3 injections spaced 2-4 weeks apart for optimal results, though many experience significant relief after a single injection. The effects typically last 3-6 months, and some patients achieve long-term or permanent relief after completing a course. When pain returns, additional injections can be administered as maintenance therapy, preventing you from escalating to stronger medications or surgery. This conservative treatment approach has helped many of our New York patients successfully manage chronic pain while maintaining active, functional lives.
Risks and Safety
Epidural steroid injections are among the safest interventional procedures available. Serious complications are extremely rare when performed by experienced physicians using fluoroscopic guidance. Minor side effects such as transient leg pain, headache, or increased pain lasting 24-48 hours occur in a small percentage of patients and resolve on their own. Infection, bleeding, and nerve damage are exceptionally uncommon due to strict sterile technique and precise needle placement. Dr. Movshis will review your medical history and any medications to ensure you’re an appropriate candidate, and we take every precaution to maximize safety and optimize your outcome.