Modal Pain’s approach to occipital nerve blocks
At Modal Pain Management, occipital nerve blocks are one of our most commonly performed headache interventions. Dr. Alexander Movshis performs every block personally — using either careful landmark technique at the superior nuchal line or, when anatomy demands, ultrasound or fluoroscopic guidance. This page explains the anatomy that matters, the conditions that respond, the real-world duration of relief, and when an occipital nerve block is the right first step versus when a different procedure is more appropriate.
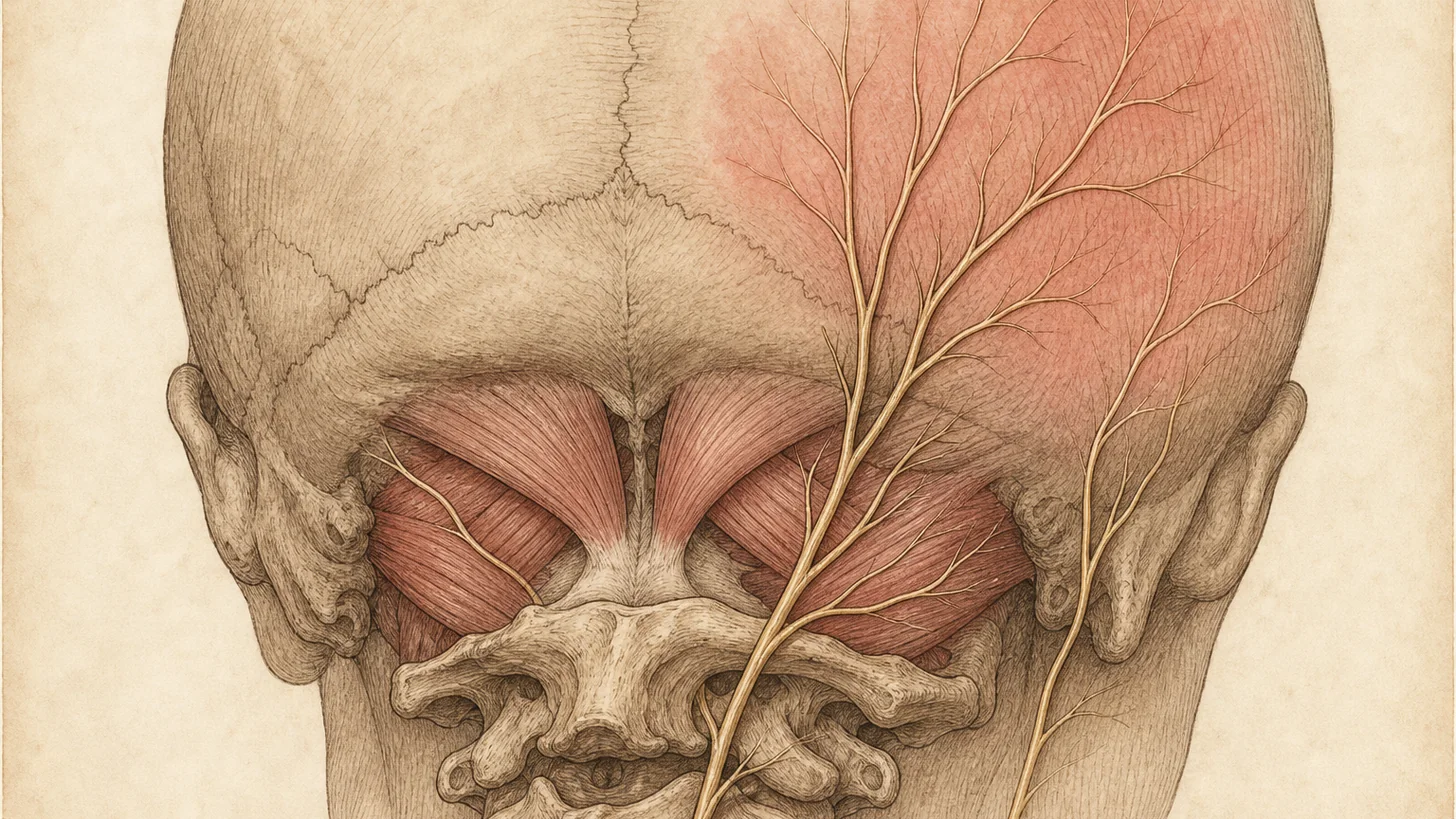
The relevant anatomy
Three sensory nerves innervate the back of the head and upper neck. All three can be blocked to control different headache syndromes:
Greater occipital nerve (GON). The dorsal ramus of the C2 spinal nerve, the GON pierces the semispinalis capitis and trapezius muscles to emerge medial to the occipital artery at the superior nuchal line. It supplies sensation to most of the posterior scalp. The GON is implicated in occipital neuralgia and in the modulation of chronic migraine and cluster headache through its convergence onto second-order neurons in the trigeminocervical complex.
Lesser occipital nerve (LON). A branch of the cervical plexus (C2–C3), the LON runs along the posterior border of the sternocleidomastoid and supplies sensation to the posterolateral scalp behind the ear. It is often blocked together with the GON in patients whose headache distribution extends laterally.
Third occipital nerve (TON). The medial branch of the C3 dorsal ramus, the TON innervates the C2–C3 facet joint and a small area of occipital scalp. Selective TON blocks are the diagnostic pathway for cervicogenic headache arising from the C2–C3 facet — and a positive TON block is the gateway to durable third occipital nerve radiofrequency ablation.
The conditions we treat with occipital nerve blocks
Occipital neuralgia. The classic indication. Patients describe sharp, shooting, or electric pain radiating from the suboccipital region up over the back of the head, sometimes behind the eye. Tinel sign over the GON is usually positive. Occipital neuralgia responds well to ONB with local anesthetic plus corticosteroid; a typical patient gains 4–10 weeks of substantial relief per injection.
Chronic migraine. For migraine that has failed two or more preventive medications, ONBs are an evidence-based adjunct, particularly when the examination reveals occipital tenderness or allodynia over the GON. RCT data (including Cuadrado 2017 and Inan 2001) show meaningful reductions in headache days and severity over 4–8 weeks. ONBs are often used alongside — not instead of — migraine preventives like Botox, CGRP monoclonal antibodies, topiramate, and beta-blockers.
Cluster headache. During an active cluster period, a GON block with corticosteroid serves as a rapid “bridge” that can break the cluster while preventives (verapamil, galcanezumab) reach steady state. Ambrosini (2005) and Leroux (2011) support this protocol.
Cervicogenic headache. Headache referred from the upper cervical spine. A TON block is diagnostic: if a fluoroscopically-guided TON injection produces same-day substantial relief, C2–C3 facet pathology is confirmed and third occipital nerve radiofrequency ablation becomes the durable next step (6–12 months of relief per ablation).
Post-concussive headache. Many post-concussive headaches have an occipital component from cervical whiplash and GON sensitization. ONBs can be a high-value intervention alongside vestibular rehab and targeted cervical physical therapy.
Other indications. Post-craniotomy pain, certain chemotherapy-induced headaches, and medication overuse headache as part of a detox strategy.
What an occipital nerve block is not
ONBs are not a diagnostic or therapeutic option for primary tension-type headache (where the pathology is cervical and paraspinal muscle, not the occipital nerve), sinus headache, or intracranial pathology. Before we perform a block, we confirm the diagnosis is one of the responsive syndromes above. If imaging is warranted (red flags, new-onset headache after age 50, progressive neurologic signs), we order it before proceeding.
The Modal Pain occipital nerve block procedure
Step 1 — Targeted history and exam. We localize the painful nerve by palpation, identify Tinel sign, and map the pain distribution to GON, LON, TON, or a combination. The physical exam drives which nerve or nerves we block.
Step 2 — Skin prep and positioning. You sit upright leaning forward, or prone for TON blocks. The posterior scalp is prepped with chlorhexidine.
Step 3 — Targeting. For GON: the nerve is identified medial to the occipital artery at the superior nuchal line, approximately one-third of the distance from the external occipital protuberance to the mastoid. We palpate the occipital artery to avoid intravascular injection. For LON: posterior to the mastoid, along the posterior border of the sternocleidomastoid. For TON: under fluoroscopic guidance at the C2–C3 facet joint.
Step 4 — Injection. A 25-gauge needle advances to the correct depth. We aspirate — if blood returns, we reposition. Then 2–4 mL of local anesthetic (lidocaine 1–2% or bupivacaine 0.25–0.5%) is delivered, with or without 10–20 mg of triamcinolone or 4–6 mg of dexamethasone. Dexamethasone is non-particulate and is increasingly preferred near the spinal axis.
Step 5 — Immediate assessment. Within 5–15 minutes we reassess the pain. Substantial reduction confirms the targeted nerve is a meaningful pain generator — this is the diagnostic signal. You go home and track symptoms over the following days and weeks.
How we decide what comes next
If an initial ONB produces meaningful but short-lived relief — say, 1–3 weeks — and the diagnosis is chronic migraine or occipital neuralgia, we repeat the block at 8–12 week intervals as part of a long-term plan.
If the initial block produces strong same-day relief but wears off in hours, and the diagnosis is cervicogenic headache with a positive TON target, we plan third occipital nerve radiofrequency ablation — a 6–12 month solution.
If the block produces no meaningful relief, we do not repeat blindly. We reexamine the diagnosis, consider peripheral nerve stimulation evaluation for refractory occipital neuralgia, and coordinate with neurology on preventive optimization.
Combining occipital nerve blocks with other treatments
ONBs complement rather than replace comprehensive headache care. We routinely coordinate with neurology on concurrent Botox for chronic migraine, CGRP monoclonal antibodies, and preventive medications. For post-concussive and cervicogenic patients, physical therapy for cervical spine mobility and deep cervical flexor strengthening is essential. For cluster patients, ONBs are a bridge — not a long-term plan — to verapamil or galcanezumab steady-state effect.
We do not combine ONBs with same-day intramuscular steroid injections in other sites, because the cumulative systemic steroid exposure becomes clinically relevant. We space procedures intentionally.
Insurance and access
Occipital nerve blocks are covered by the vast majority of commercial plans for appropriate diagnoses. Modal Pain Management accepts most major commercial PPO plans and does not accept Medicare, Medicaid, HMO plans, or workers’ compensation. Fluoroscopic third occipital nerve (TON) block capability remains relatively scarce in NYC outpatient settings — Modal Pain Management performs both ONB and TON blocks on-site under image guidance.
Verify insurance and schedule or call (646) 290-6660. Same-week consultation appointments are typically available for new patients.
Our practice difference
Dr. Movshis is a fellowship-trained pain physician who performs every occipital and third occipital nerve block personally. We do not delegate to PAs or NPs. We insist on fluoroscopic guidance for TON blocks because blind cervical spine injections are not an acceptable standard for a nerve immediately adjacent to the vertebral artery and dural sac. We follow up directly to reassess response at 2–4 weeks and decide together whether to continue, ablate, or redirect. Our goal is durable headache control, not indefinite injections on a treadmill.
Selected references
Cuadrado ML et al. Short-term effects of greater occipital nerve blocks in chronic migraine: a double-blind, randomised, placebo-controlled clinical trial. Cephalalgia. 2017;37(9):864-872.
Inan N et al. Greater occipital nerve blockade for the treatment of chronic migraine: a randomized, multicenter, double-blind, and placebo-controlled study. Acta Neurol Scand. 2001;104:155-159.
Ashkenazi A et al. Greater occipital nerve block using local anaesthetics alone or with triamcinolone for transformed migraine: a randomised comparative study. J Neurol Neurosurg Psychiatry. 2008;79(4):415-417.
Blumenfeld A et al. Expert consensus recommendations for the performance of peripheral nerve blocks for headaches — a narrative review. Headache. 2013;53(3):437-446.
Ambrosini A et al. Suboccipital injection with a mixture of rapid- and long-acting steroids in cluster headache: a double-blind placebo-controlled study. Pain. 2005;118(1-2):92-96.
Leroux E et al. Suboccipital steroid injections for transitional treatment of patients with more than two cluster headache attacks per day: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2011;10(10):891-897.
Tobin J, Flitman S. Occipital nerve blocks: when and what to inject? Headache. 2009;49(10):1521-1533.
Naja Z et al. Occipital nerve blockade for cervicogenic headache: a double-blind randomized controlled clinical trial. Pain Pract. 2006;6(2):89-95.