At Modal Pain Management in Midtown Manhattan, Dr. Alex Movshis performs medial branch blocks as the diagnostic gateway to long-term facet joint pain treatment. A medial branch block is a precision diagnostic injection that uses a small volume of local anesthetic to temporarily silence the medial branch nerve — the small sensory nerve that carries pain signals from a specific spinal facet joint. By measuring how much your familiar pain decreases during the anesthetic window, the procedure objectively confirms whether the facet joint at that spinal level is the dominant source of your pain. A positive response makes you a candidate for radiofrequency ablation (RFA), which can deliver six to twelve months or more of sustained relief from the same pain pattern. Located at 369 Lexington Avenue Floor 25 in NYC 10017, we perform medial branch blocks under live fluoroscopic guidance using the dual-block paradigm recommended by the major interventional pain societies.
What a Medial Branch Block Is — and What It Isn’t
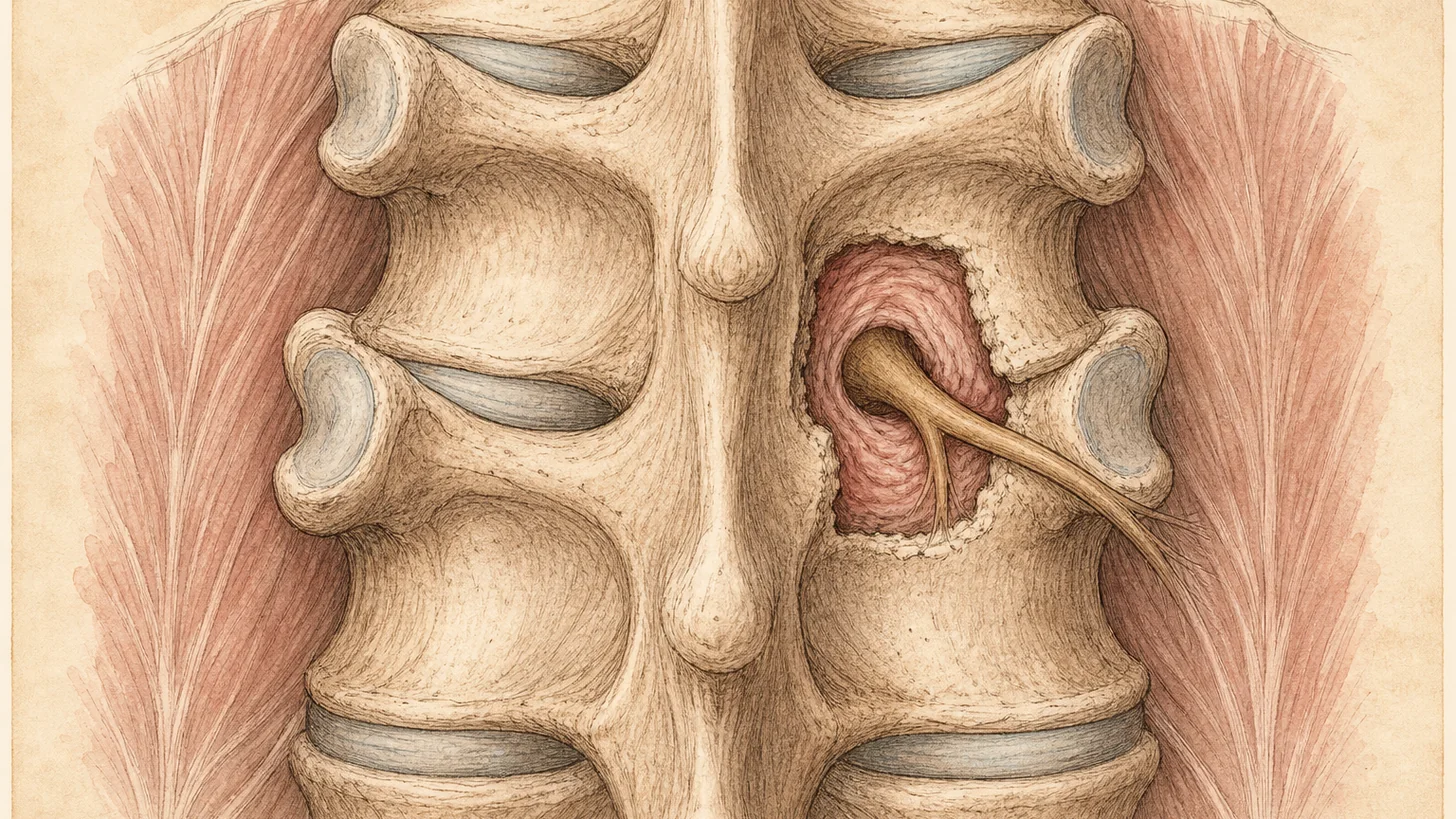
A medial branch block is fundamentally a diagnostic test, not a therapeutic injection. The medial branch nerve is the small sensory branch of the dorsal ramus that supplies each spinal facet joint with pain fibers. Each facet joint is innervated by two medial branch nerves — one from the spinal level above and one from the same level — which is why a typical block targets two nerves to evaluate a single joint. By injecting a tiny volume of short-acting local anesthetic (usually 0.5 mL of 0.5% bupivacaine per nerve) directly onto these nerves under live X-ray guidance, the procedure creates a temporary, anatomically-precise interruption of pain signaling from one specific facet joint. If your familiar pain decreases by 50% or more during the anesthetic window, the test is positive: the facet joint at that level is the source. If pain does not decrease, the test is negative and the workup moves to other potential pain generators. Unlike a cortisone injection, which is designed to reduce inflammation and provide weeks-to-months of therapeutic relief, the medial branch block is engineered to be short-lived — its diagnostic value comes precisely from its short duration.
Why Medial Branch Blocks Matter for Facet Joint Pain
Facet joint pain — clinically called facet arthropathy or zygapophyseal joint syndrome — is one of the most under-diagnosed sources of chronic back and neck pain. By age 60, roughly 50–80% of adults have measurable degenerative changes in their lumbar facet joints on imaging, but imaging alone cannot confirm whether those changes are causing pain. Many patients with facet-mediated pain have been told their MRI is “normal” or shows only “age-appropriate changes” because the dominant pathology is functional rather than structural. The clinical signature of facet joint pain — axial (centered) low back or neck pain that worsens with extension, rotation, prolonged standing, or transitioning from sitting to standing, and that does not radiate below the knee or elbow — is suggestive but not diagnostic on its own. The medial branch block is the only objective test that can confirm facet involvement, and confirming the diagnosis matters because the most durable treatment for confirmed facet pain — radiofrequency ablation — requires this objective confirmation to be safe, ethical, and insurance-approved.
Conditions Treated and Anatomic Levels
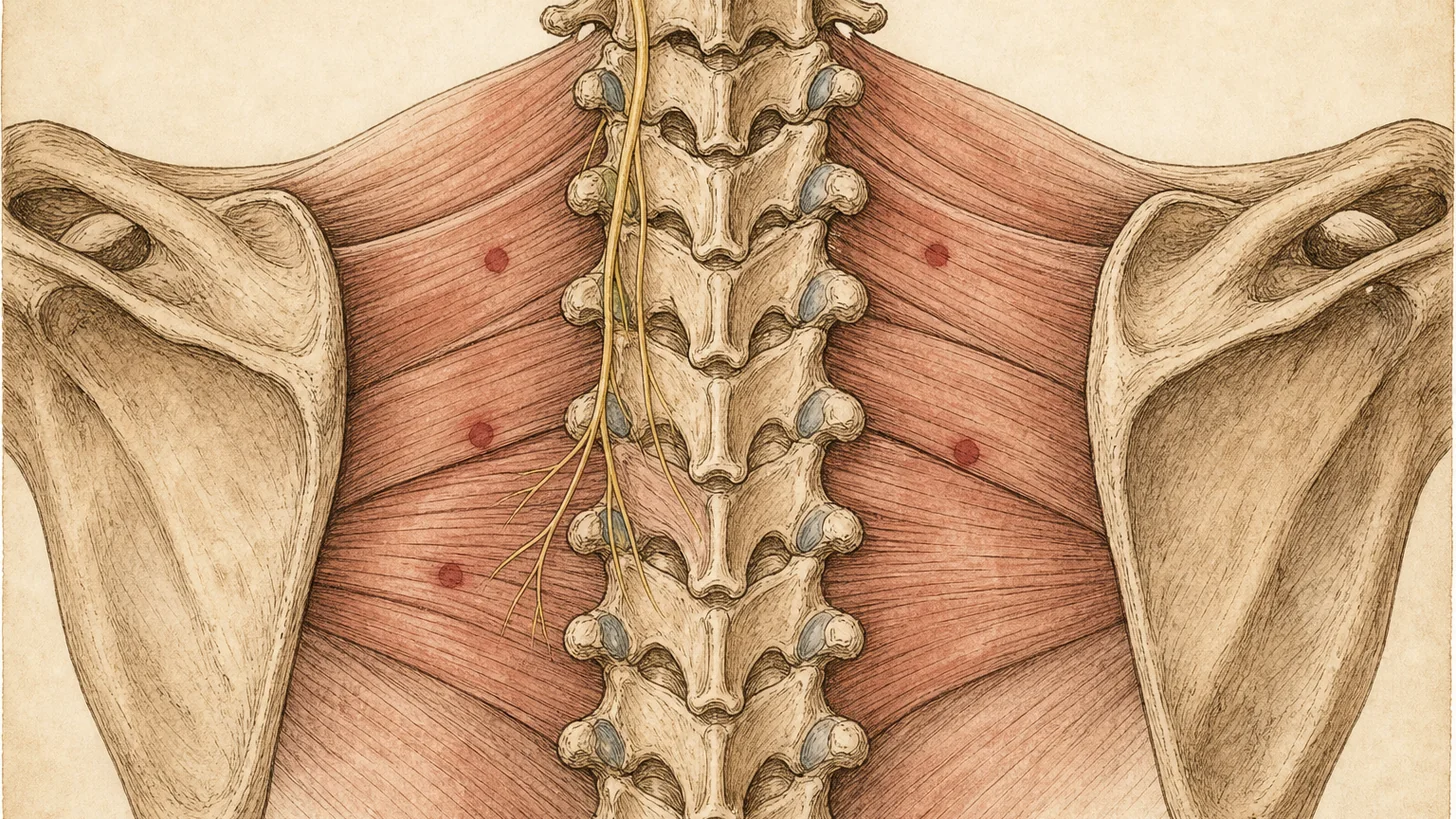
Medial branch blocks are most commonly performed in the lumbar spine (L3, L4, and L5 medial branches innervating the L4-L5 and L5-S1 facet joints) and the cervical spine (C3, C4, C5, C6, and C7 medial branches and the third occipital nerve, which innervates the C2-C3 facet joint and is a common source of cervicogenic headache). Thoracic medial branch blocks are performed less frequently but are appropriate for confirmed mid-back facet pain. Conditions evaluated and treated through this pathway include facet joint osteoarthritis, post-traumatic facet pain (often after motor vehicle collisions or falls), facet pain from spondylolisthesis, cervicogenic headache traced to the upper cervical facets, and chronic axial back pain that has not responded to a course of conservative care including physical therapy, oral medications, and activity modification. Patients with a primarily radicular pattern — pain radiating into the leg below the knee or down the arm into the hand — are evaluated for nerve root pathology with epidural steroid injections instead, since their pain is unlikely to be facet-mediated.
The Diagnostic Process: Why Two Blocks?
The dual-block paradigm — performing two separate diagnostic medial branch blocks before approving radiofrequency ablation — is the current standard of care endorsed by the International Spine Intervention Society and required by most commercial insurers. The reason is statistical. A single positive medial branch block has a false-positive rate of 25–40%, meaning that roughly one in three patients who report 50% or more pain relief from a single block do not actually have facet-mediated pain (the relief came from systemic anesthetic effect, placebo, or temporal coincidence). Two consecutive positive blocks at the same level reduce the false-positive rate to roughly 10–15%, which is the threshold at which proceeding to ablation is statistically defensible. The two blocks are typically performed 2–6 weeks apart, often using local anesthetics with different durations of action (lidocaine for one, bupivacaine for the other) to add an extra layer of confirmation. Both blocks must produce 50% or more pain relief during their respective anesthetic windows for a patient to qualify for radiofrequency ablation.
What to Expect During the Procedure
You will be positioned prone on a fluoroscopy table — face down for lumbar blocks, face down with your forehead supported for cervical blocks. The skin overlying the target spinal level is sterilized with chlorhexidine and a sterile drape is applied. A small amount of lidocaine is injected to numb the skin and superficial soft tissues — this is the only injection most patients describe as uncomfortable. Under live fluoroscopic guidance, Dr. Movshis advances a fine 22- or 25-gauge needle to the precise junction between the transverse process and superior articular process at the target level — the anatomic location of the medial branch nerve. Needle position is confirmed with a small volume of contrast dye, which on live X-ray shows the characteristic “blush” pattern that confirms the needle tip is in the correct space and not in a vessel. Once position is confirmed, 0.5 mL of local anesthetic is slowly injected. The needle is withdrawn, the process is repeated for the second medial branch nerve at the same level, and a small bandage is applied. Total procedure time is typically 20–30 minutes for a single-joint workup. No IV sedation is used in most cases, allowing patients to participate in real-time feedback about needle position and to drive themselves home.
Measuring the Response: The Pain Diary
The 4–8 hours immediately following the procedure are the most important diagnostic window. Patients are given a structured pain diary and instructed to record their pain on a 0–10 scale every 30–60 minutes for 4–8 hours, along with notes about specific activities (sitting, standing, walking, extension, rotation) that normally trigger their pain. This is critical because the entire diagnostic value of the block rests on the magnitude of pain reduction during the anesthetic window — not on whether you “felt better” overall. We ask patients to deliberately reproduce the activities and positions that normally cause their pain (within reason and safety) so we can measure whether those provocative movements still hurt during the anesthetic window. A 50% or greater reduction in your familiar pain during this window is considered a positive response. The pain diary is reviewed at your follow-up appointment 1–2 weeks after the procedure, when a treatment decision is made.
What Happens After a Positive Block
If your first medial branch block produces 50% or more pain relief during the anesthetic window, you are scheduled for a second confirmatory block at the same spinal level, typically 2–6 weeks later. If the second block also produces 50% or more pain relief, you become a candidate for radiofrequency ablation (RFA) — a procedure that uses controlled heat to create a precise lesion on the same medial branch nerves you just blocked, providing 6–12 months or more of sustained pain relief. RFA is performed in a similar way to the medial branch block (fluoroscopic guidance, prone positioning, local anesthesia) but takes slightly longer (45–60 minutes) and uses a specialized needle that delivers radiofrequency energy to create the lesion. Patients who do well with their first cycle of RFA typically maintain pain relief for 6–18 months and can have the procedure repeated when the nerve regenerates and pain returns. Learn more about the followup procedure on our radiofrequency ablation page.
What Happens After a Negative Block
If your first medial branch block does not produce at least 50% pain relief during the anesthetic window, the facet joints at that level are unlikely to be the dominant source of your pain — a useful and clinically important finding. The workup then redirects to other potential pain generators based on your history, examination, and imaging. Common next steps include investigating disc-mediated (discogenic) pain, nerve root pathology with cervical or lumbar epidural steroid injections, sacroiliac joint dysfunction with diagnostic SI joint injection, or a primarily myofascial pain source treated with trigger point injections. A negative block is not a wasted procedure — it provides objective evidence that protects you from undergoing RFA that wouldn’t have worked, and it sharpens the rest of the diagnostic workup.
How Medial Branch Block Differs from Other Spine Injections
Patients are often confused about how medial branch blocks compare to other interventional procedures, and the distinction matters because each procedure answers a different clinical question. A medial branch block uses local anesthetic only, targets the small sensory nerve to a single facet joint, is diagnostic in intent, and produces 4–24 hours of relief. An epidural steroid injection delivers steroid into the epidural space to reduce inflammation around irritated nerve roots, is therapeutic in intent, and is most appropriate for radicular pain (sciatica, cervical radiculopathy) rather than axial facet pain. An intra-articular facet joint injection delivers steroid directly into the joint capsule itself, is sometimes used both diagnostically and therapeutically, but is less anatomically precise than a medial branch block and is generally reserved for younger patients with acute facet inflammation. Radiofrequency ablation is the long-term therapeutic followup to a positive medial branch block — same target nerve, very different effect on its function. Choosing the right procedure depends on what your pain pattern, examination, and imaging suggest, which is why a structured consultation precedes any interventional procedure at our practice.
Insurance, Authorization, and Practical Logistics
Most commercial PPO insurance plans cover medial branch blocks as part of a structured workup for chronic axial back or neck pain. Coverage typically requires prior authorization, which means your plan needs documentation that you have completed a course of conservative care (usually physical therapy and oral medications) and that your clinical picture is consistent with facet-mediated pain. Modal Pain Management handles the prior authorization process on your behalf — the typical timeline is 5–10 business days from your initial consultation to authorization, and we usually schedule the procedure within the following week. We accept most major commercial PPO plans (United Healthcare, Aetna, Cigna, BlueCross BlueShield, Oxford, Empire BCBS) and do not accept Medicare, Medicaid, HMO plans, or workers’ compensation. Out-of-pocket cost depends on your individual deductible and coinsurance — we verify your benefits and provide a written estimate before your first visit so there are no surprises. Visit our insurance verification page to check your plan, or call (646) 290-6660 for a benefits check.
Why Patients Choose Modal Pain Management for Medial Branch Blocks
Dr. Alex Movshis is board-certified in Anesthesiology with subspecialty fellowship training in Interventional Pain Medicine, and performs medial branch blocks under live fluoroscopic guidance — the standard of care endorsed by the International Spine Intervention Society. Our Midtown NYC office at 369 Lexington Avenue Floor 25 is one block from Grand Central Terminal, making it accessible from anywhere in the New York metro area, and we offer same-week consultation appointments for new patients. We use the dual-block paradigm in every case to protect patients from false-positive workups, and we stage the diagnostic and therapeutic procedures (medial branch block followed by radiofrequency ablation) as a coordinated pathway rather than a series of disconnected appointments. If you have been living with chronic axial back or neck pain, have completed a course of conservative care, and want an objective answer about whether your facet joints are the source — and a clear plan for what comes next — a medial branch block is the right next step.