If you are asking which injection is best for your lower back pain, you are asking the right question — and the honest answer is that it depends on what is actually generating your pain. There are at least six evidence-based interventional procedures used for lower back pain in 2026, and they are not interchangeable. Picking the wrong one wastes time, money, and your willingness to try again. This guide is how a board-certified interventional pain physician thinks through the decision, written in plain language so you can have an informed conversation with your own doctor.
A quick note on framing. The right question is rarely “which shot will fix my back?” It is “what is causing my pain, and which procedure best matches that source?” Inflammation around a nerve root from a herniated disc behaves differently from arthritis in a facet joint, which behaves differently from sacroiliac joint dysfunction, which behaves differently from a trigger point in the paraspinal muscles. The procedure follows the diagnosis — not the other way around.
How a Pain Specialist Actually Picks the Right Injection
Before recommending any injection, a thoughtful interventional pain physician answers three questions:
Where is the pain coming from? Radicular pain that shoots into the leg suggests nerve-root inflammation. Pain that worsens with backward bending and is localized over the spine suggests facet joints. One-sided low-back pain near the dimple of Venus that worsens with sitting suggests the sacroiliac joint. Diffuse muscle pain with palpable tender knots suggests a myofascial source.
What does the imaging show? A focused MRI clarifies which structures are inflamed, compressed, or arthritic. The best procedures align an imaging finding with a matching exam finding.
What is the goal of this specific procedure? Some procedures are diagnostic — designed to confirm or rule out a pain source. Others are therapeutic — designed to provide weeks to months of relief. A few do both. Knowing the goal up front sets honest expectations.
With that framework, here are the six injections most commonly used for lower back pain, in the order a specialist typically considers them.
1. Lumbar Epidural Steroid Injection (ESI)
Best for: Radicular pain — sciatica, shooting leg pain, pain from a herniated disc, lumbar spinal stenosis, foraminal stenosis. Pain that follows a nerve-root pattern (L4, L5, or S1) into the buttock, thigh, calf, or foot.
How it works: Under fluoroscopic X-ray guidance, a needle is advanced into the epidural space surrounding the spinal cord and nerve roots. A corticosteroid (typically dexamethasone or methylprednisolone) plus local anesthetic is injected to reduce inflammation around the affected nerve root. Three approaches exist — interlaminar, transforaminal, and caudal — and the choice depends on your imaging.
Evidence and duration: Meaningful relief in approximately 50–80% of appropriately selected patients. Average duration 3–6 months, with a subset achieving permanent improvement after a short series of one to three injections.
What comes next: Pair with structured physical therapy. If two consecutive injections produce no benefit, the diagnosis should be reconsidered.
Read more: Epidural steroid injections at Modal Pain Management.
2. Medial Branch Block
Best for: Axial low-back pain (no leg radiation) that worsens with backward bending, twisting, or transitioning from sitting to standing. Pain that is reproducible over a specific spinal segment on exam. The medial branch block is primarily a diagnostic procedure — it answers the question “is your pain coming from your facet joints?”
How it works: A small volume of local anesthetic (about 0.5 mL) is placed under fluoroscopic guidance onto the medial branch nerves at two adjacent levels. You then complete a structured pain diary over the next 4–8 hours. If your usual pain drops by 80% or more, the facet joints at those levels are confirmed as the source.
Evidence and duration: Diagnostic accuracy is excellent when performed with the dual-block protocol (two positive blocks reduce false positives from 25–40% down to 10–15%). Therapeutic relief from the block itself lasts only 4–8 hours by design.
What comes next: Two positive medial branch blocks open the door to radiofrequency ablation, which provides long-lasting relief.
Read more: Medial branch block at Modal Pain Management.
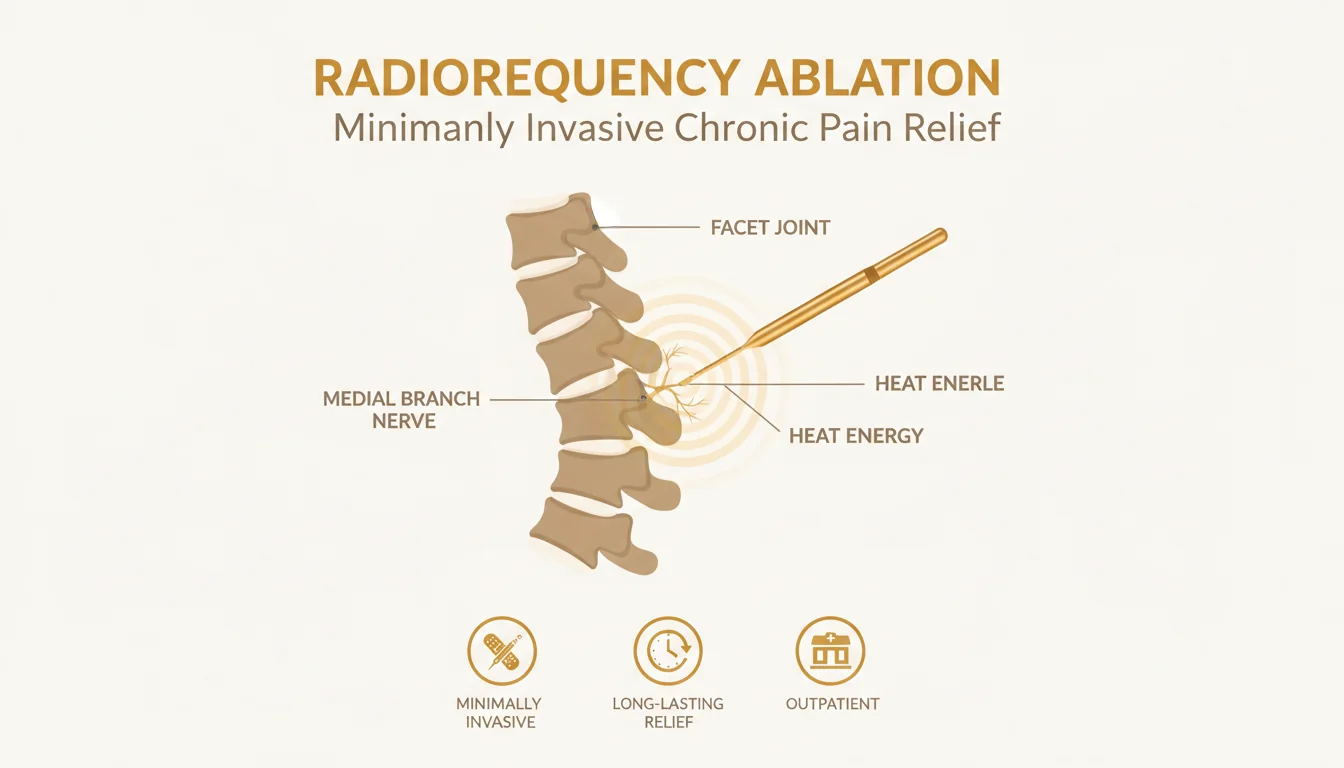
3. Radiofrequency Ablation (RFA)
Best for: Patients with confirmed facet-joint pain (two positive medial branch blocks). RFA is the long-term solution to the diagnostic question that the medial branch block answered.
How it works: Under fluoroscopic guidance, a thin probe is advanced to the medial branch nerve. Radiofrequency energy heats the probe tip, creating a small thermal lesion that interrupts the nerve’s ability to transmit pain signals. No medication is injected.
Evidence and duration: 60–80% of patients with positive diagnostic blocks experience 6–12 months of meaningful relief, sometimes longer. The medial branch nerves eventually regenerate, and RFA can be repeated as needed.
What comes next: Maintenance physical therapy and core strengthening prolong the benefit.
Read more: Radiofrequency ablation at Modal Pain Management.
4. Facet Joint Injection (Intra-Articular)
Best for: Patients with suspected facet-joint pain who are not yet candidates for the medial branch block / RFA pathway, or for whom intra-articular steroid is the better fit (acute facet inflammation, recent injury).
How it works: Under fluoroscopic guidance, a needle is placed directly into the facet joint capsule, and a corticosteroid plus local anesthetic is injected.
Evidence and duration: Variable — meaningful relief in roughly 40–60% of patients, lasting weeks to several months. The medial branch block / RFA pathway tends to outperform repeated intra-articular injections for chronic facet pain.
Most NYC interventional pain practices, including Modal Pain Management, use the medial branch block / RFA pathway as the preferred long-term strategy for confirmed facet pain.
5. Sacroiliac Joint Injection
Best for: One-sided low-back pain over the dimple of Venus that worsens with sitting, standing on one leg, climbing stairs, or transitioning from sit to stand. Often seen after pregnancy, fall onto the buttock, fusion surgery above the SI joint, or with inflammatory arthritis.
How it works: Under fluoroscopic guidance, a needle is advanced into the SI joint capsule, and a corticosteroid plus local anesthetic is injected. Like the medial branch block, the SI joint injection is both diagnostic (does pain drop after the local anesthetic?) and therapeutic.
Evidence and duration: Meaningful relief in 60–70% of patients with confirmed SI joint pain, typically lasting 3–6 months. Repeat injections can be performed as needed; some patients ultimately benefit from sacroiliac radiofrequency ablation.
Read more: Joint and soft-tissue injections at Modal Pain Management.
6. Trigger Point Injection
Best for: Myofascial pain — palpable tender knots in the paraspinal, quadratus lumborum, gluteal, or piriformis muscles. Often co-exists with one of the structural causes above and is missed when only spine imaging is reviewed.
How it works: A small needle is advanced directly into the trigger point. Lidocaine or bupivacaine is injected; some practices add a small dose of corticosteroid for inflammatory components. No imaging guidance is typically required.
Evidence and duration: Many patients experience immediate relief with sustained benefit for weeks to months, especially when paired with stretching, dry-needling, or physical therapy.
Read more: Trigger point injections at Modal Pain Management.
Quick Comparators You May Have Searched For
Nerve block vs. epidural for back pain. An epidural treats multiple nerve roots at once via the epidural space — best for radicular pain. A medial branch nerve block targets specific facet-joint nerves to confirm a facet source — best for axial pain that worsens with extension. Neither is “better” in the abstract; they answer different anatomic questions.
Cortisone shot vs. epidural. All epidural steroid injections are cortisone shots — they use a corticosteroid medication. But not every cortisone shot is an epidural; cortisone is also used in joints, bursae, and trigger points. The clinical difference is the target tissue, not the medication.
Steroid vs. PRP for back pain. Corticosteroids reduce inflammation quickly but do not regenerate tissue. Platelet-rich plasma (PRP) is being studied for facet, sacroiliac, and disc pathology with mixed but evolving evidence; it is generally considered when steroid responses have plateaued or for patients who want to avoid repeated steroid exposure.
When You Should Not Get an Injection
A spine injection is not the right next step if you have:
- New onset of leg weakness, foot drop, or saddle anesthesia (numbness in the groin) — these are surgical red flags requiring immediate evaluation
- Active infection at the injection site or systemic infection
- Unexplained fevers, weight loss, or night pain — these warrant a workup for non-mechanical causes (infection, malignancy, inflammatory arthritis) before injection
- Severely uncontrolled diabetes or anticoagulation issues that have not been addressed with your prescribing physician
- Pain that has not yet been characterized — without a working diagnosis, injecting “somewhere in the back” is poor practice
Any reputable interventional pain physician will defer the injection until these are resolved.
What to Look For in an NYC Pain Specialist
The interventional pain field has wide variability in training and practice quality. When you are choosing where to have a spine injection in New York City, ask:
- Is the physician board-certified in pain medicine (typically through anesthesiology, PM&R, or neurology), not just board-certified in their primary specialty?
- Are procedures performed with fluoroscopic guidance (live X-ray)? Blind injections in the back are not standard of care in 2026.
- Is the physician willing to explain why this specific injection matches your specific pain generator — not just offer the procedure they happen to do?
- Is there a clear next-step plan if the first injection does not work?
- Does the practice work with your insurance, and will they verify benefits before the visit?
If the answer to any of these is unclear, get a second opinion before scheduling.
The Modal Pain Management Approach
At Modal Pain Management in Midtown Manhattan, Dr. Alex Movshis is dual board-certified in anesthesiology and interventional pain management, fellowship-trained at the Icahn School of Medicine at Mount Sinai. Every injection is performed under fluoroscopic guidance in our office-based practice. Before any procedure, Dr. Movshis reviews your imaging, examines the spine, and explains in plain language which injection makes sense for your specific pain pattern — and what we will do if it does not work.
We accept most commercial PPO plans and verify your benefits before your visit at no charge. We do not accept Medicare, Medicaid, HMO plans, or workers’ compensation.
If you have lower back pain and want a clear-headed second opinion on which injection actually fits your situation, call (646) 290-6660 or book a consultation online. You will leave the visit knowing exactly what is causing your pain — and exactly what your options are.
Frequently Asked Questions
There is no single 'best' injection — the right choice depends on what is actually generating your pain. For radicular pain (sciatica, shooting leg pain from a herniated disc or spinal stenosis), a lumbar epidural steroid injection is typically first-line. For axial low-back pain that worsens with backward bending and is reproduced over a single spinal segment, a medial branch block confirms the facet joint as the source and opens the door to long-term relief with radiofrequency ablation. For one-sided low-back pain near the dimple of Venus that worsens with sitting or standing on one leg, a sacroiliac joint injection is more appropriate. The right injection is the one that matches your pain generator on physical exam and imaging — and a good pain specialist will explain that reasoning to you in plain English before any procedure.
Less than most people expect. Modern interventional pain procedures use a thin local-anesthetic needle to numb the skin and deeper tissue before the injection needle is advanced — most patients describe the deeper sensation as pressure or a brief sting rather than sharp pain. Procedures are performed under fluoroscopic X-ray guidance in 10–20 minutes, without general anesthesia. The most common discomfort is the brief skin-numbing injection itself. Patients with a strong needle aversion can request mild oral anxiolysis ahead of the visit. After the procedure, a transient pain flare lasting 24–48 hours is normal as the local anesthetic wears off and before the steroid begins to work.
It depends on the procedure. Diagnostic blocks (medial branch blocks, selective nerve root blocks, sacroiliac blocks) use a small volume of local anesthetic — typically 0.5 to 1 mL of bupivacaine or lidocaine — to confirm a pain generator. Therapeutic injections (epidural steroid injections, intra-articular facet injections, sacroiliac joint injections, joint and bursa injections) combine a corticosteroid such as dexamethasone, methylprednisolone, or triamcinolone with a local anesthetic to reduce inflammation. Trigger point injections typically use lidocaine or bupivacaine alone. Radiofrequency ablation does not inject medication — it uses heat energy delivered through a probe to interrupt pain signals from the nerves that supply painful facet joints.
Yes, but not for long. Most patients are advised to take it easy for the rest of the procedure day — gentle walking is encouraged, but avoid strenuous exercise, heavy lifting over 10–15 pounds, prolonged driving, or impact activity for 24–48 hours. You can typically return to a sedentary job the next day. The local anesthetic gives near-immediate pain relief that can create a false sense of capability for a few hours, but the steroid itself takes 2 to 7 days to reach maximum effect. A short rest window protects the injection site, allows the medication to concentrate where it was placed, and reduces the small risk of post-procedure pain flare.
An epidural steroid injection delivers anti-inflammatory medication into the epidural space surrounding the spinal cord, treating multiple nerve roots at once — best for radicular pain like sciatica from a herniated disc or spinal stenosis. A nerve block targets a specific nerve. The most common nerve block for axial low-back pain is the medial branch block, which silences the small medial branch nerves that carry pain signals from the facet joints. The decision is anatomic: epidural for nerve-root inflammation, nerve block for facet-joint or peripheral-nerve pain. Both are performed under fluoroscopy and both are diagnostic and therapeutic — but they answer different clinical questions.
An epidural steroid injection is one specific kind of cortisone shot. 'Cortisone' is shorthand for the corticosteroid medication class that includes dexamethasone, methylprednisolone, triamcinolone, and others — these medications are used in nearly every steroid injection. The difference is anatomic: an epidural injection places the corticosteroid into the epidural space around the spinal cord and nerve roots; a 'cortisone shot' for a knee, shoulder, hip, or trigger point places the same medication class into a different target for a different condition. So all epidural injections are cortisone shots, but most cortisone shots are not epidurals.
Duration varies by injection type and underlying pathology. A lumbar epidural steroid injection typically provides 3–6 months of meaningful relief, with a meaningful subset of patients achieving longer or even permanent improvement after one injection or a short series. Diagnostic medial branch blocks last only 4–8 hours by design — they are intended to confirm a pain source, not to provide lasting relief. Radiofrequency ablation, performed after two positive medial branch blocks, typically provides 6–12 months of relief and can be repeated as the nerves regenerate. Trigger point injections often relieve muscle pain for weeks to months. Sacroiliac joint injections typically last 3–6 months.