If you are reading this, you probably did everything you were asked to do. You had the surgery. You finished the chemotherapy or the radiation or both. You showed up for the follow-up appointments and the scans. The oncology side is going well. But the band of burning skin from your armpit down the inside of your arm has not faded. The bra strap hurts. Deodorant hurts. Sleeping on the affected side is impossible. Reaching overhead — for a coffee mug, for a coat, for your child — sets off a flash of electric pain that lasts seconds and that is impossible to predict.
You have been told it is normal recovery. That it will fade with time. That it is the new normal. None of that is true. The pain has a specific anatomic source, a specific diagnostic test, and a specific treatment ladder. This post is about each of those, in plain language, and why a 15-minute ultrasound-guided block usually gives the diagnostic answer in the room.
Why this gets missed
Post-mastectomy intercostobrachial neuralgia gets missed for three reasons that compound each other.
First, the published prevalence is the wrong number to anchor on. Most patients hear “5–10% of mastectomy patients develop chronic pain” from their surgical team because that is the rate of severe, function-limiting pain published in the older literature. The modern reality is that post-mastectomy pain syndrome affects roughly 25–60% of patients after breast surgery, with the intercostobrachial nerve a principal generator [1]; a prospective study at a tertiary cancer center found a post-mastectomy pain syndrome rate of about 36% at six months, most often in the anterior chest wall, axilla, and medial upper arm [3]. Many of these patients develop persistent intercostobrachial-distribution sensory disturbance — burning, allodynia, hypersensitivity to clothing. A meaningful fraction of those patients meet criteria for chronic post-surgical pain. Calling the rate “rare” sets the patient up for a system in which their pain is the unexpected exception rather than the under-served common case.
Second, the diagnostic test is not standard in oncology follow-up. Surveillance visits focus on cancer recurrence — physical examination, imaging, tumor markers. A burning band of skin in the intercostobrachial distribution does not show up on a mammogram, an MRI, or a PET-CT. A normal recurrence workup is treated as a green light. The diagnostic block that would actually identify intercostobrachial neuralgia is performed at a pain medicine practice with image-guided procedural infrastructure. Most patients are never referred for that block. A prospective cohort study of women undergoing breast cancer surgery identified handling of the intercostobrachial nerve, severe acute postoperative pain, and neuropathic signs in the first week as predictors of persistent pain at one year [2], and a 2023 review catalogued the interventional options — intercostobrachial nerve blocks among them — that become available once the nerve is identified [1]. Systematic peripheral-nerve evaluation has still not been broadly adopted in oncology follow-up.
Third, the dominant treatment paradigm is medication. Patients are prescribed gabapentin or pregabalin, often with a tricyclic antidepressant added. For some patients this produces meaningful relief. For most patients with significant intercostobrachial pain, medication alone is incomplete — the nerve injury is mechanical and structural, and medications modulate symptoms rather than addressing the generator. When medication fails, the patient is told there are no further options, when in fact image-guided block, pulsed RFA, peripheral nerve stimulation, and modern surgical neuroma management are all available paths.
The diagnostic workflow that solves this: cutaneous mapping (the patient draws the painful territory on a body diagram — a band from the axilla to the medial elbow is intercostobrachial until proven otherwise), Tinel testing along the axilla and surgical scar (positive Tinel points are common after axillary dissection), and an ultrasound-guided intercostobrachial nerve block at the axillary fascia. One visit, diagnostic answer in 30 minutes.
The anatomy that matters
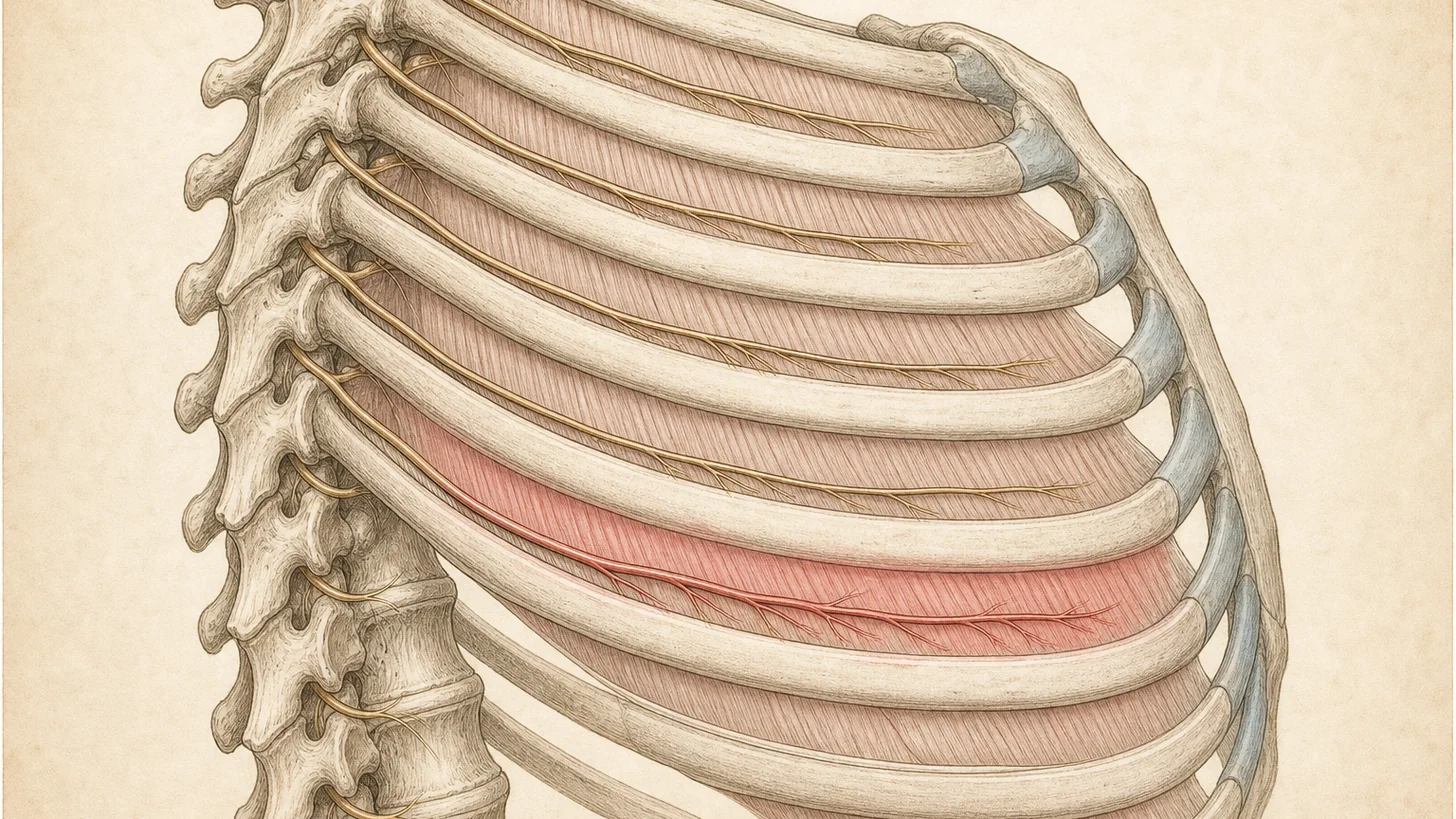
The intercostobrachial nerve is the lateral cutaneous branch of T1, with variable contributions from T2 and T3 in many patients. It originates from the second intercostal nerve, exits the second intercostal space at the midaxillary line, crosses the axillary fat pad, and supplies sensation to:
- The skin of the axilla
- The upper medial aspect of the arm, from the axilla down to and just past the elbow
- A strip of the upper medial chest wall
The clinical relevance: during axillary lymph node dissection (ALND), the intercostobrachial nerve runs directly through the surgical field. It can be transected during careful lymph node clearance, stretched during axillary retraction, or thermally injured during electrocautery dissection. Modern surgical technique increasingly attempts to preserve the nerve when oncologically safe, but a meaningful fraction of patients still develop iatrogenic neuropathy. During sentinel lymph node biopsy (SLNB) the dissection is more limited, but the intercostobrachial nerve can be sacrificed when it lies in the path of the sentinel node or when bleeding requires more extensive dissection.
Two adjacent nerves matter for the broader post-mastectomy pain picture:
- The intercostal nerves T3–T6 supply the chest wall medial to the intercostobrachial territory. They can be injured by the mastectomy incision itself, by tissue expander placement, or by implant pocket dissection. The resulting intercostal neuralgia produces a band of pain on the chest wall — distinct cutaneous distribution from the axilla-to-elbow intercostobrachial band.
- The long thoracic nerve (serratus anterior) and the thoracodorsal nerve (latissimus dorsi) are motor nerves that can be injured during ALND. Injury produces motor deficits (winged scapula for long thoracic, latissimus weakness for thoracodorsal) rather than the burning skin pattern of intercostobrachial neuralgia.
When a patient describes a band of burning from armpit to elbow that respects the medial-arm distribution and that becomes painful with bra and clothing pressure, the working diagnosis is intercostobrachial neuralgia until a diagnostic block proves otherwise.
How we diagnose
The diagnostic procedure is an ultrasound-guided intercostobrachial nerve block at the axillary fascia. Performed in our procedure suite at 369 Lexington Avenue. Total visit time: about 30 minutes.
Technique: with the patient supine and the affected arm abducted 90°, the axillary anatomy is identified by ultrasound — pectoralis major and minor anteriorly, latissimus dorsi posteriorly, the brachial plexus and axillary vessels medially, the axillary fat pad in the center. The intercostobrachial nerve is generally too small to visualize directly with standard musculoskeletal ultrasound, but its course through the axillary fascia is reliable. A 22-gauge needle is advanced under direct ultrasound visualization into the axillary fascia just lateral to the pectoralis major margin, at the level of the second-third intercostal space. After negative aspiration, 4–5 mL of 0.5% bupivacaine plus 20–40 mg of triamcinolone is delivered, with spread observed in real time as a hypoechoic plane within the axillary fascia.
The diagnostic effect is immediate. Within 10–15 minutes, the band of burning pain should abolish or substantially decrease. ≥50% pain abolition is positive; ≥75% is highly specific. The patient keeps a pain diary every 30 minutes for the next four hours and at intervals over the next several days.
The therapeutic effect with corticosteroid added typically lasts 4–12 weeks. For patients with a clear positive response and diminishing duration on repeat blocks, the next step is pulsed radiofrequency ablation of the intercostobrachial nerve — pulsed (not conventional thermal) RFA because the territory innervated is cosmetically sensitive and the lesion must be neuromodulatory rather than destructive. Pulsed RFA typically delivers 6–12 months of relief and is safely repeatable.
For patients with broader post-mastectomy pain — concurrent intercostal neuralgia, scar-bound neuromas, or shoulder adhesive capsulitis — sequential diagnostic blocks identify each component, and the treatment ladder is built around the dominant generator first.
Treatment ladder and when surgery is the right call
Step 1 — neuropathic-pain medication. Most patients with significant post-mastectomy pain have already been on gabapentin, pregabalin, or duloxetine before they reach an interventional pain practice. We refine the trial — adequate dose titration, addition of a tricyclic at low dose if not yet tried, topical 5% lidocaine patch over the affected band for focal cutaneous relief.
Step 2 — ultrasound-guided diagnostic and therapeutic nerve block. The workhorse described above. Diagnostic in 15 minutes, therapeutic for 4–12 weeks with steroid.
Step 3 — ultrasound-guided neuroma injection. For palpable or sonographically-identified neuromas at the mastectomy scar, direct corticosteroid plus local anesthetic injection produces durable relief in many patients; chemical neurolysis with dilute phenol or alcohol is an option for refractory neuromas before surgical excision.
Step 4 — stellate ganglion block. For patients with allodynia plus color/temperature change in the affected territory (suggesting a sympathetically-maintained component), stellate ganglion block under ultrasound guidance is diagnostic and therapeutic.
Step 5 — pulsed radiofrequency ablation of the intercostobrachial or affected intercostal nerves. For 6–12 months of relief at a time, repeatable as the nerve regenerates.
Step 6 — peripheral nerve stimulation referral. Percutaneous PNS at the intercostobrachial nerve is a growing option for severe refractory disease, with FDA clearance and a strong published case-series base.
Step 7 — surgical neuroma management by peripheral nerve plastic surgery. When the conservative ladder reaches its ceiling, the durable salvage is operative. Two procedures are commonly indicated:
- Targeted muscle reinnervation (TMR) — the proximal nerve stump is coapted to a motor nerve of a small expendable muscle, giving the regenerating axon a productive target rather than letting it form another disorganized neuroma. Originally developed for amputation neuromas, TMR has been adapted for chronic peripheral neuropathic pain including post-mastectomy intercostobrachial neuralgia. Published case series show meaningful pain reduction in 70–85% of selected patients.
- Regenerative peripheral nerve interface (RPNI) — the proximal nerve stump is implanted into a small denervated muscle graft. Functions analogously to TMR. Both are performed by peripheral nerve plastic surgery teams in specialized programs.
For all surgical referrals, Modal Pain coordinates the handoff directly and provides the surgical team with the documented diagnostic-block response, prior operative report from the mastectomy, oncology and radiation history, and any imaging — the documentation that surgical neurectomy programs require to accept a referral.
For the broader framework on post-mastectomy pain across mechanisms, see the post-mastectomy pain syndrome page.
For referring physicians
When referring a post-mastectomy patient with persistent chest-wall, axillary, or upper-arm pain >3 months after surgery, send: the operative report (mastectomy type, axillary intervention — SLNB vs. ALND, reconstruction approach), the radiation oncology course summary if relevant, the patient's medication trial history, and a note on the dominant cutaneous distribution (axilla-to-elbow band points to intercostobrachial; chest-wall band points to intercostal; focal Tinel point points to scar neuroma). We document a sensory map at the consultation, run an ultrasound-guided intercostobrachial diagnostic block at the axillary fascia, and send notes back to the referring surgical and oncology teams after each visit. For refractory cases that meet criteria, we coordinate the peripheral nerve plastic surgery referral for RPNI or TMR.
Ready to evaluate your post-mastectomy pain
If your post-mastectomy pain has persisted more than three months and standard oncology follow-up has not produced a treatment path for it, the next step is an image-guided diagnostic intercostobrachial block. Same-week new-patient consultations are available at 369 Lexington Avenue in Midtown Manhattan.
Verify your insurance covers a post-mastectomy pain workup Book a same-week diagnostic block
Or call (646) 290-6660.
For the broader framework on post-surgical nerve pain across surgical contexts, see the post-surgical and iatrogenic nerve pain pillar.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Murugappan A, Khanna A. Interventional Treatment Options for Post-mastectomy Pain. Current Oncology Reports. 2023;25(10):1175-1179. doi:10.1007/s11912-023-01435-z · PubMed
- Andersen KG, Duriaud HM, Jensen HE, Kroman N, Kehlet H. Predictive factors for the development of persistent pain after breast cancer surgery. Pain. 2015;156(12):2413-2422. doi:10.1097/j.pain.0000000000000298 · PubMed
- Kakati B, Nair N, Chatterjee A. Post mastectomy pain syndrome at an Indian tertiary cancer centre and its impact on quality of life. Indian Journal of Cancer. 2023;60(2):275-281. doi:10.4103/ijc.ijc_861_21 · PubMed
Frequently Asked Questions
Most patients notice the first symptoms within 4–12 weeks after surgery. Some patients experience early relief in the first few months and then a delayed onset 6–18 months later, often as the surgical bed continues to remodel. About 25–60% of patients who have mastectomy with axillary lymph node dissection develop persistent intercostobrachial neuralgia (rate depends on surgical extent), and a smaller but meaningful subset of patients after sentinel lymph node biopsy alone develop it when the intercostobrachial nerve has been sacrificed.
The intercostobrachial nerve supplies a band of skin from the axilla down the medial upper arm to the elbow. The bra strap and underwire sit directly over this territory. When the nerve is injured during surgery, that territory develops allodynia — light touch becomes painful. Common irritants are bra straps, deodorant application, the back of a chair, a partner's hand on the upper arm, the inside of a sleeve. The mechanical trigger is not the cause; the underlying nerve injury is. The bra strap is just delivering the stimulus to a nerve that should not feel painful to gentle touch.
Intercostobrachial neuralgia is the most common single mechanism behind post-mastectomy pain syndrome (PMPS), but PMPS is broader. PMPS includes intercostobrachial neuralgia, intercostal neuralgia (T3–T6 chest wall), scar neuromas, persistent post-radiation pain, and adhesive-capsulitis-pattern shoulder stiffness. Most patients with PMPS have a dominant intercostobrachial component plus one or more secondary components. The diagnostic block sorts them out — abolishing the axilla-to-elbow band of pain with an intercostobrachial block isolates that component.
A small needle is placed under ultrasound guidance into the axillary fascia. Most patients describe it as similar to a vaccination — a brief pinch, then a few seconds of pressure as the medication is injected. No IV sedation is needed. The diagnostic answer — does this block abolish the burning band — usually arrives within 15 minutes. If the block is positive, corticosteroid is included and produces 4–12 weeks of therapeutic relief.
Regenerative peripheral nerve interface (RPNI) and targeted muscle reinnervation (TMR) are modern surgical techniques developed for amputation neuromas and now applied to other refractory peripheral nerve pain. For post-mastectomy intercostobrachial neuralgia that has failed the conservative ladder (medication, blocks, hydrodissection, pulsed RFA, peripheral nerve stimulation), referral to a peripheral nerve plastic surgeon for RPNI/TMR is the durable salvage option. The procedure transects the intercostobrachial nerve proximal to the affected region and implants the proximal stump into a small denervated muscle graft, which gives the regenerating axon a productive target rather than letting it form another neuroma.
No. Intercostobrachial nerve blocks, pulsed RFA, and any subsequent peripheral nerve surgery are completely independent of your oncology care. We coordinate with your medical oncologist, radiation oncologist, and breast surgeon by sending notes after each visit, and we time interventions around active chemotherapy or radiation cycles when needed. Many patients continue active surveillance, anti-hormonal therapy (tamoxifen, aromatase inhibitors), or reconstructive surgery while being treated for intercostobrachial neuralgia.
Most commercial PPO plans cover image-guided intercostobrachial and intercostal nerve blocks for chronic post-mastectomy pain, typically with prior authorization. Pulsed RFA requires a documented positive response to one or more diagnostic blocks before approval. Modal Pain verifies your benefits before scheduling. We accept most major commercial PPO plans and do not participate with Medicare or Medicaid. <a href="/verify-insurance/">Check your plan</a> or call (646) 290-6660.