Most patients who turn out to have genitofemoral neuralgia have already been checked for a recurrent hernia — sometimes twice — and the scan was clean each time. The pain burns in the groin and shoots down into the upper thigh, there is often a raw, electric feeling in the scrotum or the labia, and none of it behaves like the dull, mechanical ache of a hernia. What they have is an injured nerve. Genitofemoral neuralgia is a well-described cause of chronic neuropathic groin pain, most often arising after surgery in the lower abdomen and groin, and it is under-recognized precisely because its territory overlaps two other nerves and because there is no lump to point to [1].
What genitofemoral neuralgia feels like
The pain follows the nerve. It usually starts in the lower abdomen or groin and spreads to the medial and upper-anterior thigh, with paresthesias and a burning quality, and in many patients it reaches the genitals — the scrotum in men, the labia majora and mons pubis in women [1]. It tends to worsen with walking, hip extension, and prolonged standing, and the overlying skin can be painfully sensitive to clothing. What it does not do is produce a bulge. A hernia is a reducible swelling that pushes out with coughing or straining and aches mechanically. Genitofemoral pain is burning and electric, it is there without any swelling, and it does not reduce because there is nothing to reduce.
The nerve and its two branches
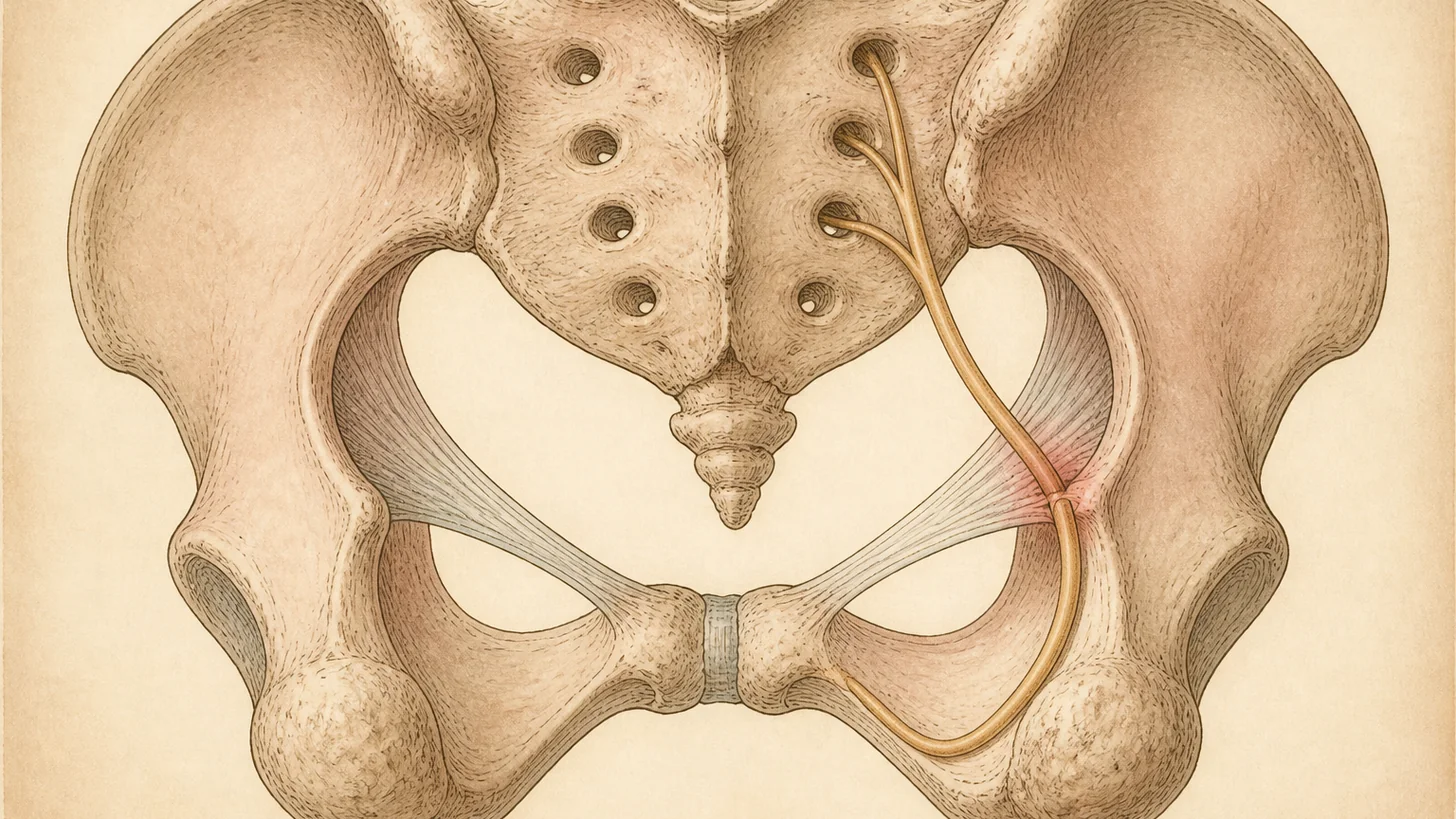
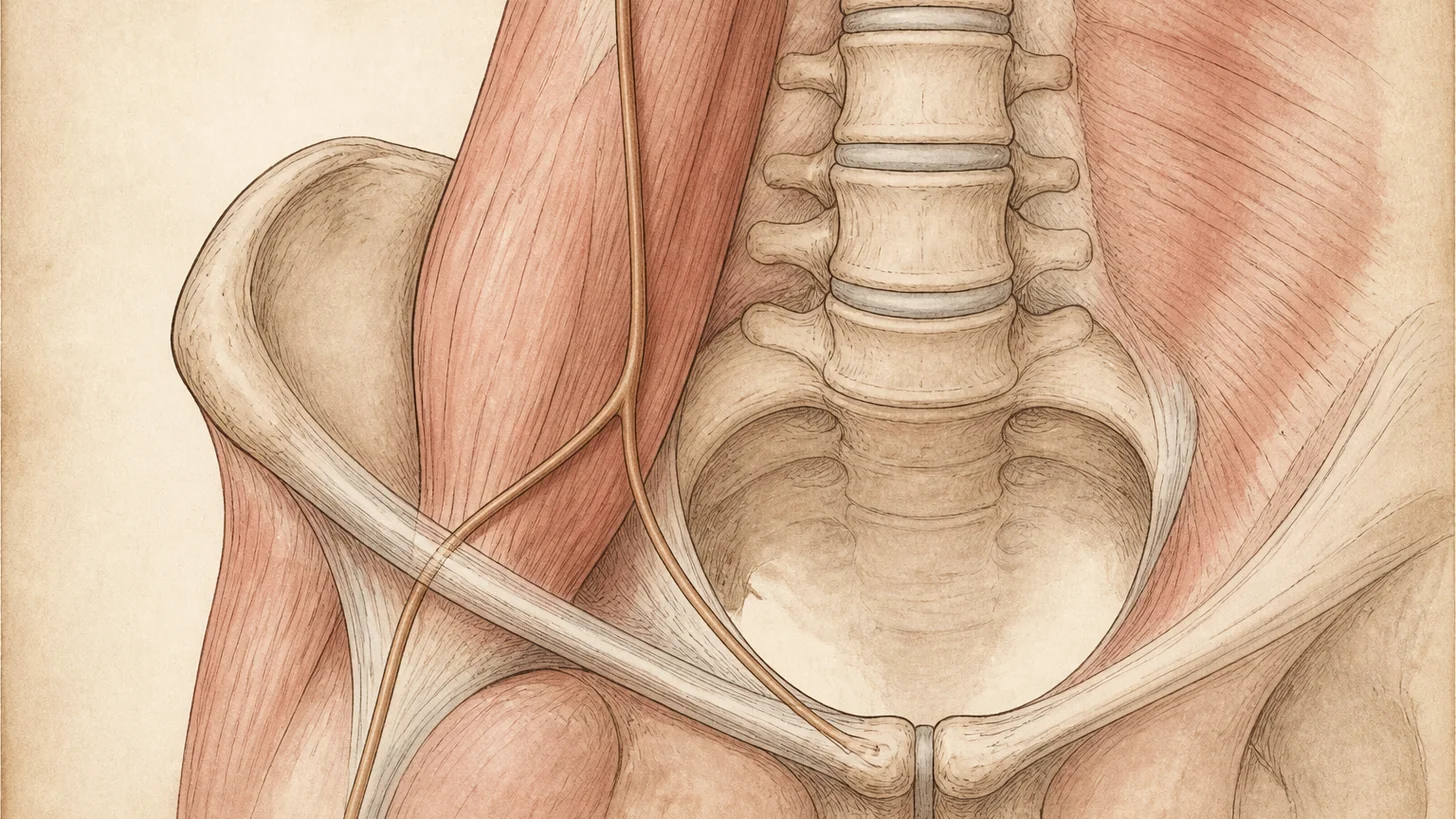
The genitofemoral nerve arises from the first and second lumbar nerve roots and runs down the front of the psoas muscle before splitting into two branches that explain the whole syndrome [1]. The genital branch enters the inguinal canal, supplies the cremaster muscle, and carries sensation from the scrotum in men or the round ligament, mons pubis, and labia majora in women. The femoral branch passes under the inguinal ligament and supplies the skin over the femoral triangle at the top of the front thigh. One nerve, therefore, covers both a patch of genital skin and a patch of thigh skin — an unusual pairing that, when it burns together, is close to a fingerprint for this nerve.
It is injured where surgery happens. Inguinal and femoral hernia repair is the classic cause, in both open and laparoscopic forms, where mesh or sutures sit against the nerve or its genital branch. Cesarean section, appendectomy, and other pelvic or retroperitoneal procedures can irritate it through retraction or scar, and trauma and pregnancy account for a few more, with a minority idiopathic [1]. The common thread is a genitofemoral nerve caught in or compressed by the aftermath of an operation.
Why it’s mistaken for a hernia — and for the wrong nerve
Two confusions send patients down the wrong path. The first is the hernia itself: groin pain after a repair is assumed to be a recurrence, and only after a clean scan does attention turn to the nerves. The second, subtler error is blaming the wrong nerve. The genitofemoral, ilioinguinal, and iliohypogastric nerves share the groin, and their cutaneous territories overlap and vary between people. In a dissection study of 64 sides, the branching pattern of the ilioinguinal and genitofemoral nerves fell into four distinct types, with the genitofemoral dominating the scrotal, labial, and ventromedial-thigh skin in some people and the ilioinguinal dominating in others [2]. You cannot reliably tell these nerves apart by where the pain is, because where the pain is depends on an anatomy that differs from patient to patient.
There is one exam sign that helps. The genital branch of the genitofemoral nerve drives the cremaster muscle, so a diminished or absent cremasteric reflex on the painful side points toward the genitofemoral nerve rather than the purely sensory ilioinguinal nerve [1]. It narrows the field, but it does not close the case — for that, the pain generator has to be switched off directly.
How genitofemoral neuralgia is diagnosed
The diagnosis is clinical, then confirmed by a block. History and exam raise the suspicion — groin-to-thigh burning, genital pain, no bulge, and a reduced cremasteric reflex. Because the three border nerves overlap, selective image-guided diagnostic nerve blocks of the genitofemoral, ilioinguinal, and iliohypogastric nerves are done to localize the pain generator rather than guessing from the map [1][2]. Imaging supports the workup: MR neurography can show the abnormal nerve and exclude other causes, and in a series of 106 patients with groin or genital pain, image-guided nerve blocks directed by MR neurography improved pain in about 84% of cases [3]. A block that reliably abolishes the familiar pain, even briefly, is worth more than any single image.
Evidence-based treatment
Treatment follows a ladder, and most patients climb only as far as they need to [1][6].
It starts conservatively, with neuropathic pain medication and physical therapy to settle the surrounding muscle and scar. When that is not enough, the genitofemoral nerve block moves from diagnosis to therapy: local anesthetic, usually with a corticosteroid, placed at the nerve under ultrasound or CT guidance. In reported cases this has produced months of relief and, repeated, has been enough to keep pain controlled alongside medication [4]. When the block helps but the relief is short, pulsed radiofrequency of the nerve is the next step — a non-destructive treatment that, in a refractory post-surgical case, resolved the pain with benefit holding at nine months [5]. These are the interventional tools a peripheral nerve entrapment practice brings to the groin, and they sit alongside radiofrequency ablation and cryoablation in the wider toolkit for nerve-driven pain [1][6].
Cases that respond to blocks but keep relapsing are candidates for a targeted neurectomy, in which the offending nerve is divided to stop the signal for good — the definitive option when a specific nerve has been proven to carry the pain [1][6]. When the pain began after a hernia repair, that surgical decision belongs in a coordinated plan with the operating surgeon, which is the focus of our note on chronic groin pain after hernia surgery.
When to see a specialist
Burning groin pain that spreads into the upper thigh or the genitals, especially after inguinal hernia repair, a Cesarean, or other lower-abdominal surgery, and especially when the hernia workup is clean and there is no bulge, deserves evaluation for genitofemoral neuralgia. Because it shares its territory with other groin and pelvic nerves, it is worth reading alongside our notes on pudendal neuralgia and the outer-thigh burning of meralgia paresthetica. The sooner the right nerve is confirmed with a block, the sooner treatment can target it instead of another round of imaging for a hernia that isn’t there.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Cesmebasi A, Yadav A, Gielecki J, Tubbs RS, Loukas M. Genitofemoral neuralgia: a review. Clinical Anatomy. 2015;28(1):128-35. doi:10.1002/ca.22481 · PubMed
- Rab M, Ebmer J, Dellon AL. Anatomic variability of the ilioinguinal and genitofemoral nerve: implications for the treatment of groin pain. Plastic and Reconstructive Surgery. 2001;108(6):1618-23. doi:10.1097/00006534-200111000-00029 · PubMed
- Poh F, Xi Y, Rozen SM, Scott KM, Hlis R, Chhabra A. Role of MR neurography in groin and genital pain: ilioinguinal, iliohypogastric, and genitofemoral neuralgia. American Journal of Roentgenology. 2019;212(3):632-43. doi:10.2214/AJR.18.20316 · PubMed
- Shanthanna H. Successful treatment of genitofemoral neuralgia using ultrasound guided injection: a case report and short review of literature. Case Reports in Anesthesiology. 2014;2014:371703. doi:10.1155/2014/371703 · PubMed
- Thapa D, Ahuja V, Verma P, Das C. Successful management of a refractory case of postoperative herniorrhaphy pain with extended duration pulsed radiofrequency. Saudi Journal of Anaesthesia. 2016;10(1):107-9. doi:10.4103/1658-354X.169488 · PubMed
- Elkins N, Hunt J, Scott KM. Neurogenic pelvic pain. Physical Medicine and Rehabilitation Clinics of North America. 2017;28(3):551-69. doi:10.1016/j.pmr.2017.03.007 · PubMed
Frequently Asked Questions
Genitofemoral neuralgia is neuropathic pain in the territory of the genitofemoral nerve — a nerve from the upper lumbar spine that supplies the skin over the femoral triangle at the top of the front thigh and, through its genital branch, the scrotum and cremaster muscle in men or the mons pubis and labia majora in women. It is a nerve problem, not a hernia, so it produces burning or electric pain without a bulge, and it does not get better with a hernia repair. The diagnosis is confirmed by a selective nerve block that switches the pain off.
Burning, shooting, or aching pain that starts in the lower abdomen or groin and spreads to the upper front and inner thigh, often with genital pain — the scrotum in men, the labia in women. It tends to flare with walking, hip extension, or prolonged standing, and the skin over the area can be hypersensitive to clothing. There is no lump to feel. Because the pain sits in the groin, it is frequently blamed on a recurrent hernia until imaging comes back clean.
Most cases are iatrogenic — the nerve is injured or entrapped during surgery in the lower abdomen and groin. Inguinal and femoral hernia repair is the classic trigger, in both open and laparoscopic techniques, but Cesarean section, appendectomy, and other pelvic or retroperitoneal operations can do the same. Trauma, scar tissue, and pregnancy are less common causes, and some cases have no clear trigger. In all of them the mechanism is the same: an irritated or trapped genitofemoral nerve.
They share territory, which is exactly why they are confused. The distinguishing signs are the genital branch's motor job and the pattern of pain. The genitofemoral nerve drives the cremaster muscle, so a diminished or absent cremasteric reflex on the affected side points to it rather than the ilioinguinal nerve, which is purely sensory in the groin. Because the cutaneous territories of these nerves overlap and vary from person to person, the reliable way to tell them apart is a selective image-guided block of each nerve in turn — the one that abolishes the pain is the culprit.
Clinically, and then confirmed with a block. The history and exam raise the suspicion — groin-to-thigh burning, genital pain, no bulge, and a reduced cremasteric reflex. Because the genitofemoral, ilioinguinal, and iliohypogastric nerves overlap, selective image-guided diagnostic blocks are done to localize the pain generator, and MR neurography can show the abnormal nerve. In one series of 106 patients with groin or genital pain, image-guided nerve blocks based on MR neurography improved pain in roughly 84% of cases.
Treatment climbs a ladder. It starts with neuropathic pain medication and physical therapy. When that is not enough, a genitofemoral nerve block — local anesthetic, often with a corticosteroid — is both diagnostic and therapeutic and can give months of relief. When the block helps but the pain returns, pulsed radiofrequency of the nerve can extend the benefit, and cryoablation is another option. Cases that respond to blocks but keep relapsing are candidates for a targeted neurectomy. The goal is to interrupt the one nerve carrying the pain without creating a new problem.