Most patients who turn out to have pudendal neuralgia arrive with a folded towel or a special cushion under one arm and a year of wrong labels behind them — prostatitis, vulvodynia, “chronic pelvic pain,” sometimes the suggestion that it is stress. They can tell you the exact number of minutes they can sit before the burning starts, and they have quietly reorganized their life around not sitting. The diagnosis is missed for years partly because the pain is in a place people are reluctant to describe, and partly because it is genuinely hard to prove — pudendal neuralgia takes many years to be recognized in a typical patient, and there is no blood test or scan that clinches it [6]. What clinches it is the pattern.
What pudendal neuralgia feels like
The pain is neuropathic — burning, aching, or a raw electric quality — in the perineum, the genitals, or around the anus, usually on one side. Its defining feature is the relationship to sitting: it increases the longer you sit and through the course of the day, and it decreases when you stand or lie down [3]. People describe sitting on a golf ball, a hard ridge, or a foreign body in the rectum or vagina. Sexual pain, a sense of incomplete or painful urination, and pain with bowel movements often ride alongside it, because the same nerve carries all of that territory [3].
Two quieter features matter for diagnosis as much as the pain itself. The pain characteristically does not wake you from sleep, and a careful sensory exam of the area comes back normal — there is no numb patch to find, even where it burns [1]. A useful everyday clue is the toilet-seat sign: sitting on a toilet seat, where the cutout offloads the perineum, hurts less than sitting on a solid chair. That single observation tells you the problem is pressure on the perineal nerve, not the pelvic organs.
The nerve and where it gets trapped
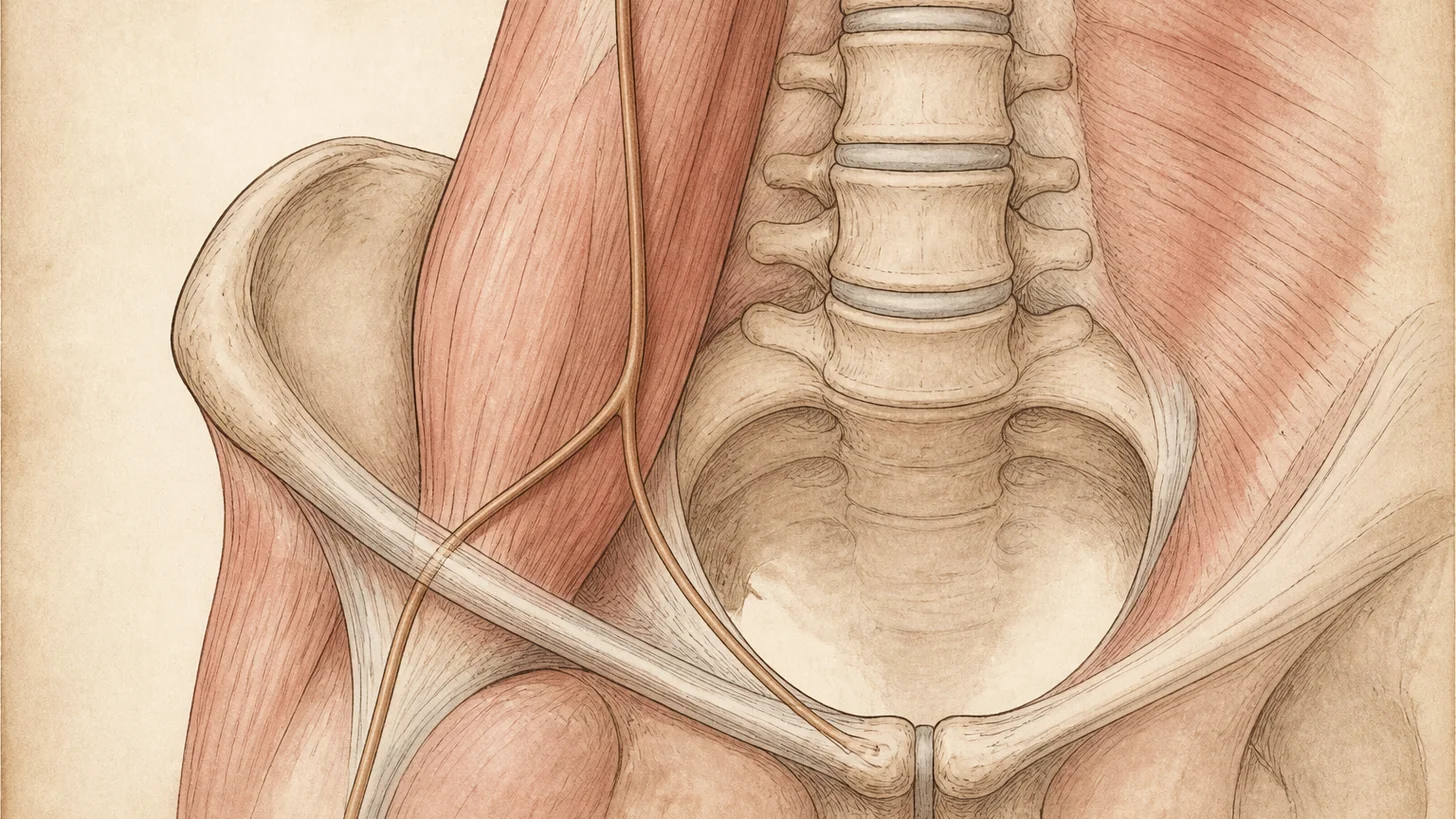
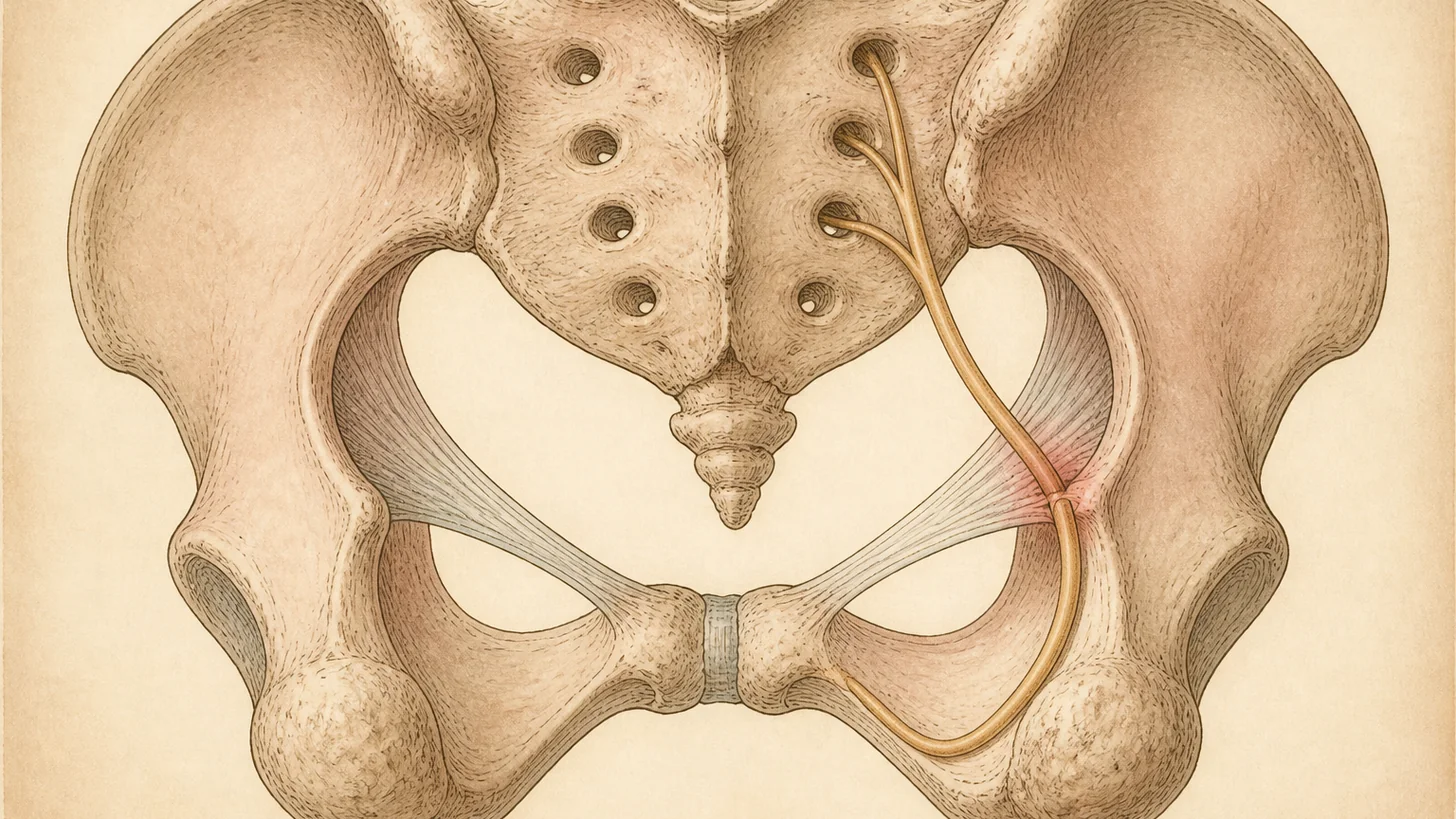
The pudendal nerve arises from the sacral roots S2, S3, and S4 [6]. It leaves the pelvis, hooks around the ischial spine, re-enters through a gap called the lesser sciatic foramen, and then runs forward in a fascial tunnel along the side wall of the pelvis known as Alcock’s (pudendal) canal. Along the way it divides into three branches — to the anus and rectum, to the perineum, and the dorsal nerve of the penis or clitoris — which is why one irritated nerve can produce pain spanning the whole area.
It gets trapped where it is tethered. In a series of 100 patients operated for pudendal neuralgia, the compression sat at the ischial spine, pinched between the sacrospinous and sacrotuberous ligaments, in roughly three-quarters of cases, with the infrapiriform foramen and Alcock’s canal accounting for most of the rest [5]. That anatomy explains the mechanics: sitting drives the nerve against the ischial spine and squeezes the ligamentous clamp tighter, so load plus time equals pain. The common triggers all fit the same theme of pressure or traction on the nerve — childbirth, pelvic and perineal surgery, intense cycling, falls onto the sit-bones, and sacroiliac or skeletal abnormalities, with a slow age-related version in some patients [3].
Why it’s misdiagnosed for years
The territory is shared with the urologist, the gynecologist, and the colorectal surgeon, so the first several workups look for a prostate, bladder, vulvar, or rectal cause and come back unrevealing. Because the nerve problem does not show on standard imaging and leaves no numb patch, a normal set of tests gets misread as “nothing wrong” rather than as evidence pointing at the nerve. The condition is uncommon on paper — often quoted at about 1 in 100,000, though clinicians who treat it think the real figure is higher [2] — which keeps it off the list of usual suspects. The result is a long detour through antibiotics for prostatitis, creams for vulvodynia, and bladder treatments, none of which touch a nerve.
How pudendal neuralgia is diagnosed
The diagnosis is clinical and rests on the Nantes criteria, a validated checklist built specifically because there is no single confirmatory test [1]. Five features are essential: pain in the territory of the pudendal nerve, pain worsened by sitting, pain that does not wake the patient at night, no objective sensory loss on examination, and relief from an anesthetic pudendal nerve block. The criteria also spell out what argues against the diagnosis — pain that is only over the tailbone, buttock, or lower abdomen, pain that comes only in fleeting jabs, itching alone, or an imaging finding that already explains the symptoms [1].
Tests play a supporting role. MRI and nerve imaging are used mainly to exclude other causes and, occasionally, to show a compressing structure, not to confirm the neuralgia itself. The diagnostic nerve block is the workhorse: because it doubles as a treatment, an image-guided block at the ischial spine or Alcock’s canal is usually the point where the workup and the management plan meet [2]. A block that reliably abolishes the pain, even briefly, is worth more than any scan.
Evidence-based treatment
Treatment is a ladder, and most patients climb only as far as they need to [3].
The first rung is unloading the nerve and calming it down. That means a seat cushion that offloads the perineum, a real break from cycling or other perineal pressure, pelvic-floor physical therapy to release the muscles that crowd the nerve, and neuropathic pain medication of the kind used for other nerve pain. Many milder or clearly triggered cases settle here.
When pain persists, the pudendal nerve block moves from diagnosis to therapy — anesthetic, usually with a corticosteroid, placed at the nerve to interrupt the pain and, in many patients, to buy a stretch of relief that outlasts the anesthetic. When that relief is real but short, pulsed radiofrequency of the same nerve is the next step: a non-destructive treatment that a systematic review found to be the most frequently used current-based technique for this condition, with reported improvements in pain and quality of life, though the authors are candid that the overall evidence base is thin [6]. These are the interventional tools a peripheral nerve entrapment practice brings to the pelvis, and they sit alongside radiofrequency ablation in the wider toolkit for nerve-driven pain.
For the subset with genuine entrapment who respond to blocks but keep relapsing, surgical decompression addresses the cause. It is the one treatment tested in a randomized controlled trial: patients randomized to decompression did markedly better than those managed without surgery — about 50% improved at three months versus 6% of controls, and by twelve months roughly 71% of the surgical group were improved against 13% of controls, with benefit holding at four years [4]. Neuromodulation, including spinal cord and nerve stimulation, is held in reserve for pain that outlasts the rest of the ladder [3][6].
When to see a specialist
Burning or aching pain in the perineum, genitals, or rectum that gets worse the longer you sit, eases when you stand, and does not wake you at night deserves evaluation for pudendal neuralgia — particularly after a urology or gynecology workup has come back clean, and especially if it followed childbirth, pelvic surgery, a fall onto the sit-bones, or heavy cycling. Because the pain shares its map with post-surgical pelvic nerve problems, it is worth reading alongside our notes on pelvic nerve pain after hysterectomy and chronic groin pain after hernia surgery. The sooner the nerve is confirmed as the source, the sooner a targeted block can replace another round of treatment aimed at the wrong organ.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourology and Urodynamics. 2008;27(4):306-10. doi:10.1002/nau.20505 · PubMed
- Hibner M, Desai N, Robertson LJ, Nour M. Pudendal neuralgia. Journal of Minimally Invasive Gynecology. 2010;17(2):148-53. doi:10.1016/j.jmig.2009.11.003 · PubMed
- Pérez-López FR, Hita-Contreras F. Management of pudendal neuralgia. Climacteric. 2014;17(6):654-6. doi:10.3109/13697137.2014.912263 · PubMed
- Robert R, Labat JJ, Bensignor M, Glemain P, Deschamps C, Raoul S, Hamel O. Decompression and transposition of the pudendal nerve in pudendal neuralgia: a randomized controlled trial and long-term evaluation. European Urology. 2005;47(3):403-8. doi:10.1016/j.eururo.2004.09.003 · PubMed
- Ploteau S, Perrouin-Verbe MA, Labat JJ, Riant T, Levesque A, Robert R. Anatomical variants of the pudendal nerve observed during a transgluteal surgical approach in a population of patients with pudendal neuralgia. Pain Physician. 2017;20(1):E137-43. PubMed
- Piñeiro-Franco L, Alonso-Calvete A, Da Cuña-Carrera I. Management of pudendal neuralgia with electrical stimulation. A systematic review. Actas Urológicas Españolas. 2024;48(6):416-26. doi:10.1016/j.acuroe.2024.02.001 · PubMed
Frequently Asked Questions
Pudendal neuralgia is neuropathic pain in the territory of the pudendal nerve — the nerve that carries sensation from the perineum, the genitals, and the area around the anus. It is a nerve problem, not a muscle, prostate, or gynecologic one, which is why it does not respond to the antibiotics or anti-inflammatories aimed at those. The hallmark is pain that is worse sitting and eased by standing, and the diagnosis rests on a clinical checklist called the Nantes criteria rather than on a scan.
Burning, aching, or a raw, electric feeling in the perineum, genitals, or rectum — usually on one side — that builds the longer you sit and lets up when you stand or lie down. Many people describe a sense of sitting on a golf ball or a folded sock, or a foreign-body feeling in the rectum or vagina. The overlying skin can be painfully sensitive, and there is often sexual, urinary, or bowel discomfort layered on top. A telling clue is that sitting on a toilet seat, which takes the weight off the perineum, hurts less than sitting on a normal chair.
The nerve is irritated, compressed, or stretched somewhere along its course. Common triggers are childbirth, pelvic or perineal surgery, prolonged or intense cycling, falls onto the tailbone or sit-bones, and skeletal or sacroiliac abnormalities, with some cases developing gradually with age. Anatomically, the nerve is most often trapped where it passes the ischial spine between two pelvic ligaments, or further along in a tunnel called Alcock's canal.
Clinically, using the Nantes criteria. The five essential features are pain in the pudendal nerve's territory, pain worse with sitting, pain that does not wake you from sleep, no measurable loss of sensation on exam, and meaningful relief from an anesthetic pudendal nerve block. Imaging is used mainly to rule out other causes rather than to confirm the diagnosis, because the nerve problem itself usually does not show up on a scan. A diagnostic pudendal nerve block that switches off the familiar pain is the single most useful test.
Treatment is layered. It starts with unloading the nerve — a cushion that offloads the perineum, stopping cycling for a while — plus pelvic-floor physical therapy and nerve-directed medication. When that is not enough, a pudendal nerve block is both diagnostic and therapeutic, and pulsed radiofrequency of the same nerve can extend relief. Cases that respond to blocks but keep relapsing are candidates for surgical decompression, which in a randomized trial relieved pain in most patients out to a year and beyond. Neuromodulation is an option for stubborn cases.
Many people get substantial, lasting relief, but there is no single overnight fix and the timeline is measured in weeks to months. Cases caught early and driven by a clear, removable trigger — a cycling habit, a specific compression — tend to do best. Longstanding cases usually improve in steps: offloading and physical therapy first, then blocks and pulsed radiofrequency, then decompression surgery if the nerve is genuinely trapped. The realistic goal is to turn pain that dominates your day into pain you can control.