Most patients who turn out to have suprascapular nerve entrapment arrive with a year of rotator cuff exercises behind them and a shoulder that is no better. The pain sits at the back and outside of the shoulder, the arm is weak turning outward, and the working diagnosis has been tendinitis or a partial cuff tear the whole time. Suprascapular neuropathy was long treated as a rare, diagnosis-of-exclusion problem, but it is recognized more often now as a real source of shoulder pain and weakness — sometimes on its own, sometimes riding alongside other shoulder pathology [1][2]. The reason it hides is anatomical: the muscles it controls are the same ones the rotator cuff exam tests, so a failing nerve and a failing tendon look alike from the outside.
What suprascapular nerve entrapment feels like
The pain is usually a deep, diffuse ache across the back and outer shoulder that patients struggle to localize with one finger. It tends to worsen with overhead activity and cross-body reaching, and it can radiate toward the neck or down the arm, which adds to the confusion with cervical and cuff problems [2][3].
Where the nerve is compressed changes the picture. Compression at the suprascapular notch, higher up, involves both the supraspinatus and infraspinatus, producing pain plus weakness of the first part of raising the arm and of turning it outward. Compression further back, at the spinoglenoid notch, spares the supraspinatus and hits the infraspinatus alone — and here the story is often painless or nearly so, with the first clue being weakness of external rotation and a visible hollow where the infraspinatus has wasted below the shoulder-blade spine [1][2]. Athletes in overhead sports — volleyball, throwing, swimming — are the classic setting for that spinoglenoid pattern.
The nerve and its two choke points
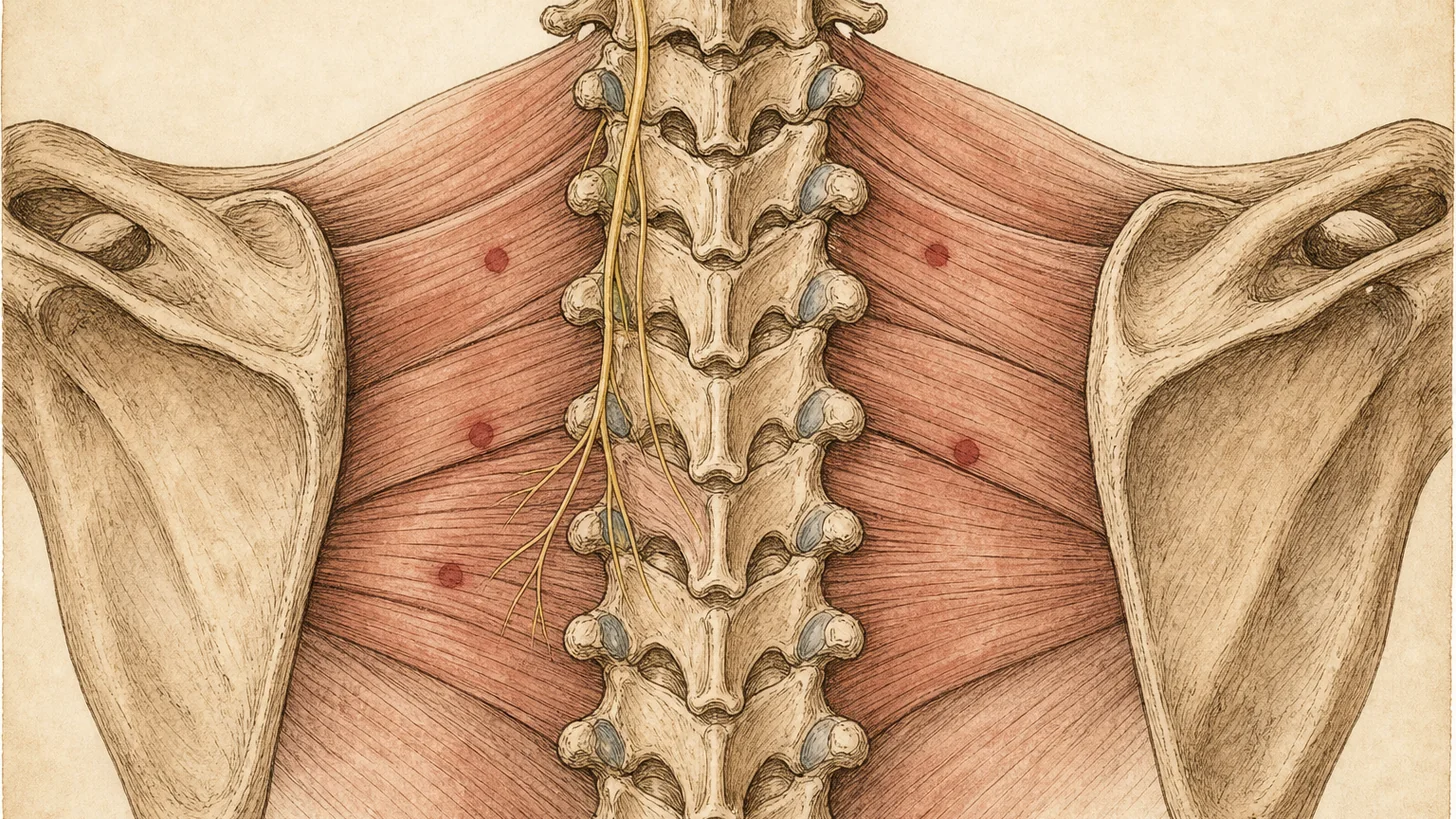
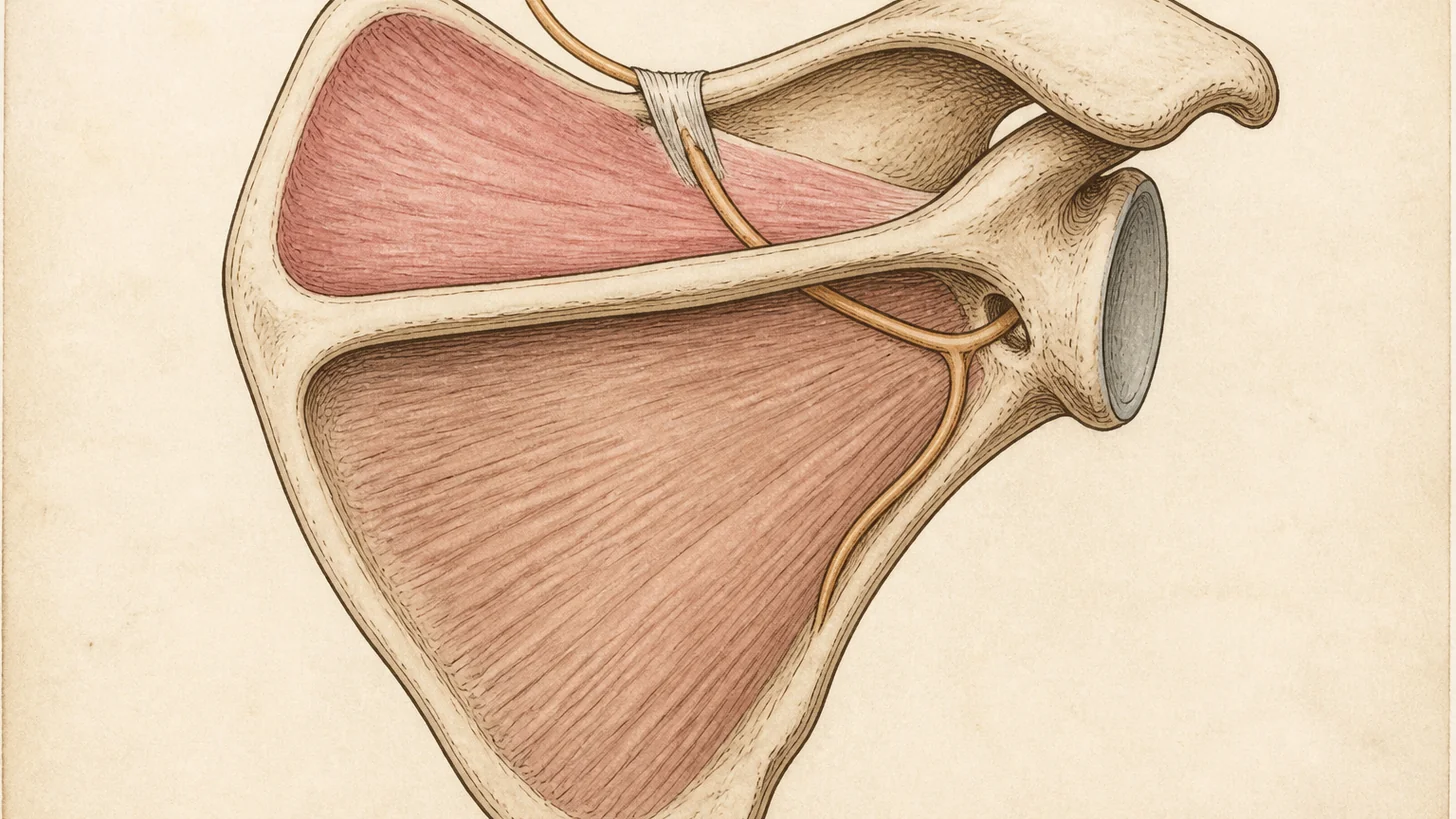
The suprascapular nerve leaves the upper trunk of the brachial plexus and runs a winding course from the base of the neck to the back of the shoulder. It passes first through the suprascapular notch, under the transverse scapular ligament, then wraps around the base of the scapular spine through the spinoglenoid notch. At both notches the nerve is tethered in a tight bony-ligamentous tunnel with little room to move, which is exactly why those two points are where it gets trapped [1][2]. Along the way it gives motor branches to the supraspinatus and infraspinatus and sensory branches to roughly 70% of the shoulder joint, including the posterior capsule and the acromioclavicular joint — the anatomical reason a block of this one nerve can quiet so much shoulder pain.
Three mechanisms account for most cases. Repetitive overhead traction stretches the nerve against these fixed points. A space-occupying cyst — most often a paralabral (ganglion) cyst that tracks out of a labral tear and lodges at the spinoglenoid notch — compresses it directly. And a large, retracted rotator cuff tear can drag the nerve medially and put it under chronic traction [1][3]. When none of these is present, the entrapment is called idiopathic.
Why it gets mistaken for a rotator cuff problem
The infraspinatus is the shared variable. It is a rotator cuff muscle, so its weakness reads as a cuff problem on exam, and external-rotation weakness is one of the first things a cuff workup looks for. The distinguishing move is to look at the muscle rather than only test it: isolated infraspinatus wasting with an intact-appearing cuff on imaging is a nerve sign, not a tendon sign. On MRI, the giveaway is either a discrete cyst at the spinoglenoid notch or a denervation pattern — edema early, fatty atrophy later — confined to the muscles a single suprascapular nerve supplies [3][4].
How suprascapular nerve entrapment is diagnosed
The workup layers three things onto the history and exam. MRI is the most useful single test — it shows a compressing cyst or mass, and it reads the muscle for the edema-then-atrophy signature of denervation that localizes the lesion to the suprascapular or spinoglenoid notch [3][4]. Ultrasound is a useful adjunct for imaging the nerve and guiding injection [4]. Electromyography and nerve conduction studies remain the confirmatory standard for a neuropathy, with the important caveat that nerve pain can be present even when the EMG is normal, so a negative study does not clear the nerve [1][3]. The suprascapular nerve block closes the loop: because it doubles as a treatment, it is usually the pivot point between working the problem up and managing it.
Evidence-based treatment
Treatment follows the cause. When there is no structural compression, care starts conservatively: activity modification to unload the overhead traction, physical therapy to restore scapular mechanics and rotator cuff balance, and anti-inflammatory medication [1][2][3]. This is the right first step for traction-type and idiopathic cases, and many settle with it.
When pain persists, the suprascapular nerve block moves from diagnosis to therapy. Local anesthetic, usually with a corticosteroid, is placed at the nerve; it relieves pain in a large share of patients and confirms the target at the same time [2][3]. When that relief is genuine but short-lived, pulsed radiofrequency of the suprascapular nerve is the next step — a non-destructive treatment that, in a prospective study of chronic shoulder pain, reduced pain and improved range of motion for at least six months [5]. These are the interventional tools a peripheral nerve entrapment practice brings to the shoulder, and they sit alongside radiofrequency ablation in the broader toolkit for nerve-driven pain.
Structural compression is treated at its source. A paralabral cyst is aspirated or decompressed; a discrete entrapment at the notch, or a case that fails conservative and interventional care, is referred for arthroscopic decompression, which reliably relieves pain in most patients even though the return of strength and muscle bulk is less predictable [1][2][3]. The dividing line is whether something is mechanically squeezing the nerve — if it is, relieving that compression comes first; if it is not, the interventional pain pathway of block and pulsed radiofrequency does the work.
When to see a specialist
Posterior shoulder pain that has not responded to months of rotator cuff rehab, weakness turning the arm outward, or a visible hollow below the shoulder-blade spine all warrant evaluation for suprascapular nerve entrapment — especially in an overhead athlete or anyone with a known labral tear. Interscapular and neck-driven pain can mimic it, so it is worth reading this alongside our note on pain between the shoulder blades. The sooner the nerve is confirmed as the source, the sooner targeted treatment can replace another round of exercises for the wrong diagnosis.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Boykin RE, Friedman DJ, Higgins LD, Warner JJP. Suprascapular neuropathy. The Journal of Bone and Joint Surgery. American Volume. 2010;92(13):2348-64. doi:10.2106/JBJS.I.01743 · PubMed
- Piasecki DP, Romeo AA, Bach BR, Nicholson GP. Suprascapular neuropathy. Journal of the American Academy of Orthopaedic Surgeons. 2009;17(11):665-76. doi:10.5435/00124635-200911000-00001 · PubMed
- Freehill MT, Shi LL, Tompson JD, Warner JJP. Suprascapular neuropathy: diagnosis and management. The Physician and Sportsmedicine. 2012;40(1):72-83. doi:10.3810/psm.2012.02.1953 · PubMed
- Mangi MD, Zadow S, Lim W. Nerve entrapment syndromes of the upper limb: a pictorial review. Insights into Imaging. 2022;13(1):166. doi:10.1186/s13244-022-01305-5 · PubMed
- Pinto RDT, Pinto JMT, Loureiro MCU, Cardoso C, Assuncao JP. Ultrasound-guided pulsed radiofrequency for chronic shoulder pain: a prospective study. Brazilian Journal of Anesthesiology. 2024;74(1):744268. doi:10.1016/j.bjane.2021.08.006 · PubMed
Frequently Asked Questions
A deep, aching, poorly localized pain across the back and outer shoulder, often worse with overhead reaching and hard to pin to one spot. When the nerve is pinched further back, at the spinoglenoid notch, the pain can be mild or absent and the first sign is weakness turning the arm outward — reaching for a seatbelt, brushing hair — along with visible hollowing of the muscle below the shoulder blade.
They overlap, which is why the nerve problem is missed. Both cause posterior shoulder pain and weak external rotation. The tell is the pattern: isolated wasting of the infraspinatus muscle with a normal-looking rotator cuff on imaging points to the nerve, and an MRI cyst at the spinoglenoid notch or a denervation pattern on the muscle confirms it. A rotator cuff tear shows a torn tendon on MRI instead.
Three common mechanisms: repetitive overhead traction on the nerve (volleyball, throwing, swimming), a space-occupying cyst — usually a paralabral (ganglion) cyst arising from a labral tear at the spinoglenoid notch — and traction from a large, retracted rotator cuff tear that drags on the nerve. Some cases have no clear cause and are considered idiopathic.
By combining the exam with imaging and, when needed, nerve testing. MRI is the most useful single test: it shows a compressing cyst and the pattern of muscle denervation or atrophy that localizes the problem to the suprascapular or spinoglenoid notch. Electromyography and nerve conduction studies are the confirmatory standard, though nerve pain can exist with a normal EMG. A diagnostic suprascapular nerve block that switches off the pain supports the diagnosis and previews which treatment will help.
Start conservatively when there is no structural compression: activity modification, physical therapy to restore scapular mechanics, and anti-inflammatory medication. When pain persists, a suprascapular nerve block is both diagnostic and therapeutic, and pulsed radiofrequency of the nerve can extend relief for months. A cyst compressing the nerve is drained or decompressed, and a discrete structural entrapment or a case that fails conservative care is referred for arthroscopic decompression.
Yes. A suprascapular nerve block places local anesthetic (often with a corticosteroid) at the nerve to interrupt the pain it carries from roughly the top and back of the shoulder joint. It relieves pain in many patients and confirms the nerve as the source at the same time. When the relief is real but short-lived, pulsed radiofrequency of the same nerve is the next step for longer-lasting control.