The most common version of this problem is mundane: a desk worker with a deep, nagging ache between the shoulder blades that builds through the afternoon, eases overnight, and has been treated as a “knot” with foam rollers and massage for months without really going away. Most of the time that is exactly what it looks like — a mechanical, postural, treatable problem. The reason to read past the foam roller is that the interscapular region is one of the few places in the back where ordinary muscle pain shares an address with a short list of serious mimics, and with a commonly missed source in the neck. Sorting those out is the whole game.
Rule out the dangerous causes first
Almost all interscapular pain is benign. The point of starting here is not to alarm — it is that the serious causes are time-sensitive, so they get ruled out at the front of the visit, not the end.
With those off the table, what remains is overwhelmingly mechanical — and that is good news, because mechanical interscapular pain is diagnosable and treatable. One caveat on location: pain that sits further out, over the shoulder blade itself, with weakness turning the arm outward, points to a different problem — suprascapular nerve entrapment, where the nerve to the back of the rotator cuff is choked rather than a muscle between the blades.
What “between the shoulder blades” actually is
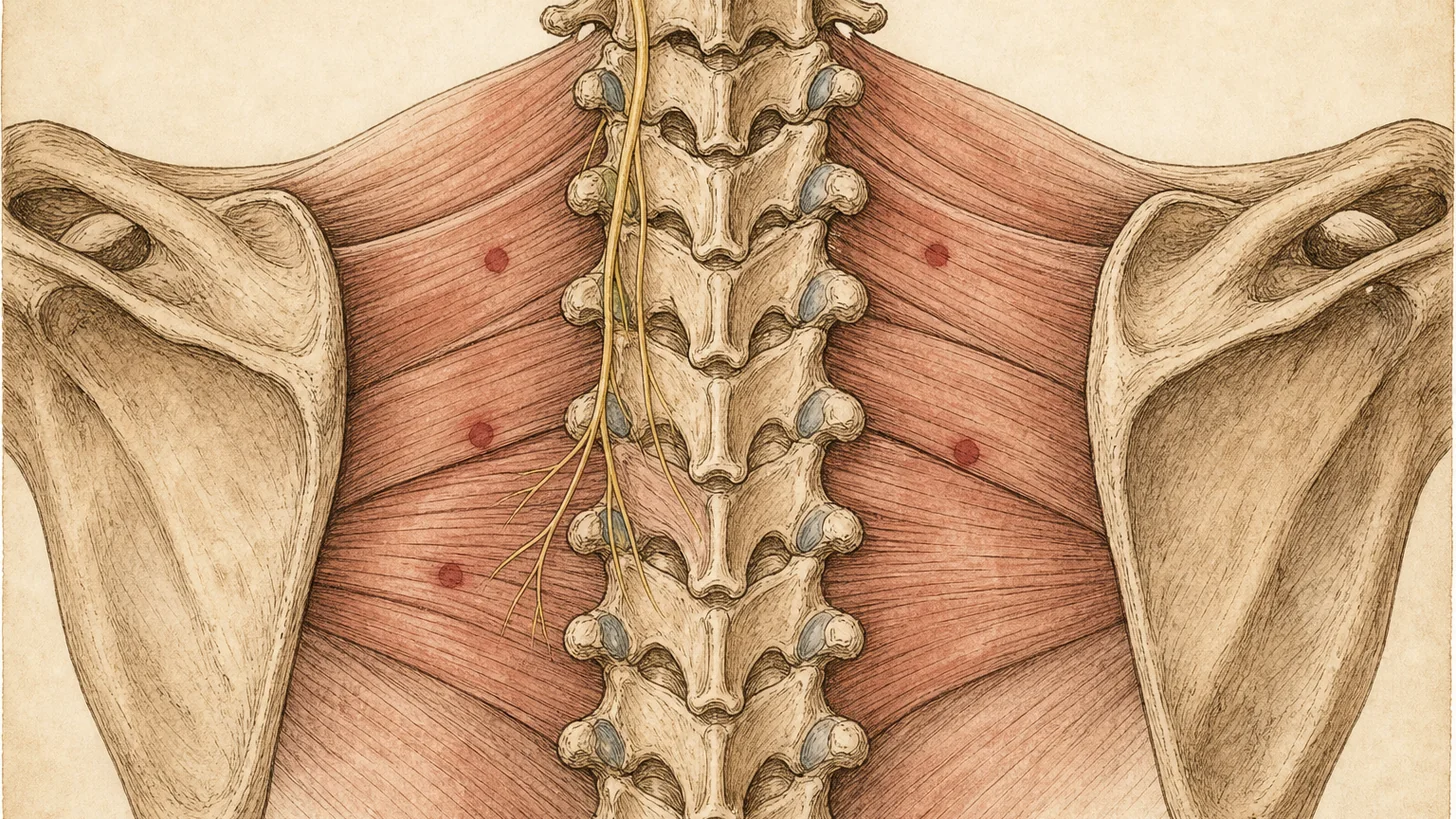
The interscapular region sits over the upper-to-mid thoracic spine, framed by the medial borders of the two shoulder blades. The structures that generate pain here are the postural muscles that hold the scapulae down and back (the rhomboids, the middle and lower trapezius, the levator scapulae), the thoracic vertebrae and their facet and rib joints, and the nerves of the cervical and thoracic spine that refer pain into this area. This is distinct from pain in the shoulder joint itself, which points to a different set of causes — covered separately in sudden shoulder pain without injury.
Thoracic spine pain is common and under-studied compared with neck and low-back pain. A systematic review of working adults found one-year prevalence clustering around 30%, with consistent associations to office work, high workload, perceived ergonomic problems, and female sex [1]. In other words, the single biggest driver is how modern work loads the upper back.
The usual causes, in order of frequency
Myofascial pain and trigger points. This is the most common source. Sustained forward-head, rounded-shoulder posture overloads the mid-trapezius and rhomboids, which develop taut bands and trigger points that ache and refer pain across the interscapular region. Myofascial pain syndrome is extraordinarily common — one review estimates it affects up to 85% of adults at some point [2]. It is also the cause most often dismissed as “just a knot,” when it is in fact a treatable pain generator. Desk posture and “tech neck” are the typical setup.
Thoracic facet and rib joints. Each thoracic vertebra connects to its neighbors through paired facet (zygapophyseal) joints and to the ribs through costovertebral and costotransverse joints. These are genuine pain generators: injecting the thoracic facet joints in healthy volunteers reproduces local and referred pain [4], and detailed mapping shows the upper thoracic joints from C7-T1 to T2-3 refer pain precisely into the suprascapular, superior scapular angle, and mid-scapular regions [3]. A facet-driven pattern is typically a deeper, more localized ache, worse with extension and rotation of the upper back.
Referred pain from the neck. This is the one most often missed. The lower cervical spine refers pain downward into the interscapular region — provocative cervical discography maps show the C3-C4, C4-C5, C5-C6, C6-C7, and C7-T1 discs all referring pain into the area between the shoulder blades [5]. The lower cervical facet joints do the same. The tell is that the interscapular pain tracks with neck position and is reproduced when the neck is examined, not when the painful spot is pressed. A person can have a “between the shoulder blades” complaint with no neck pain at all and still have a neck source. When that is the case, treating the upper back alone never works — the problem is upstream, and our neck pain evaluation is where it gets sorted.
Less common sources. A thoracic disc protrusion can produce focal or band-like pain, and early shingles can cause a burning interscapular pain for a few days before the rash appears. If the complaint is an itch more than a pain — a fixed, well-defined patch — that is a different entity, notalgia paresthetica, not muscular pain.
How it’s diagnosed
After the red-flag screen, diagnosis is clinical and mechanical. A focused history (desk hours, what aggravates and relieves it, whether it tracks with neck movement) plus an examination that tries to reproduce the familiar pain from each candidate structure — the muscles, the thoracic facets, the lower cervical spine. Imaging is reserved for red flags or a focal neurologic finding, because degenerative changes look the same on MRI whether or not they hurt. When the source is ambiguous and treatment is escalating, a diagnostic block settles it: a trigger point injection for a muscular source, or a fluoroscopically guided medial branch block of the thoracic facet (or a cervical evaluation) for a joint or referred source. The block both confirms the generator and predicts which longer-term treatment will work.
Evidence-based treatment
Treatment follows the cause.
Posture and physical therapy come first for the common musculoskeletal patterns. Targeted strengthening of the deep neck flexors and the scapular stabilizers, plus ergonomic change to the desk setup, addresses the mechanical overload that drives most interscapular pain [1]. Our physical therapy program is built around that.
Trigger point treatment when myofascial trigger points are the generator. Trigger point injections deactivate the taut band directly; for stubborn trigger points, botulinum toxin is an option — a randomized, double-blind, placebo-controlled trial found a single botulinum toxin injection raised the pressure-pain threshold in upper trapezius trigger points [6], and Modal Pain delivers it through neuromodulator injections. A broader review supports a stepped, interventional approach to myofascial pain when conservative care stalls [2].
Thoracic facet treatment when a facet joint is the confirmed source. A medial branch block confirms the target, and radiofrequency ablation of the medial branches then interrupts the pain signal for months, repeatable when the nerve regenerates [3][4].
Treat the neck when the neck is the source. If the interscapular pain is referred from the lower cervical spine, the durable fix targets that level — not the muscle that hurts [5]. This is the case the foam roller can never reach.
When to see a specialist
Most interscapular pain settles with posture work and time. Bring in an interventional pain physician when it has not responded to a few weeks of conservative care, when it keeps returning after massage or therapy that only helps briefly, or when it tracks with neck movement — the signal that the source may be upstream in the cervical spine. And act on the emergency features above without waiting: sudden severe or tearing pain, or pain with chest, breathing, or neurologic symptoms, belongs in an emergency room, not a clinic.
Verify your insurance covers an interscapular pain workup Book a same-week evaluation
Or call (646) 290-6660.
For the broader framework on upper- and mid-back pain, see the back pain page.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Briggs AM, Bragge P, Smith AJ, Govil D, Straker LM. Prevalence and associated factors for thoracic spine pain in the adult working population: a literature review. Journal of Occupational Health. 2009;51(3):177-92. doi:10.1539/joh.k8007 · PubMed
- Galasso A, Urits I, An D, et al. A Comprehensive Review of the Treatment and Management of Myofascial Pain Syndrome. Current Pain and Headache Reports. 2020;24(8):43. doi:10.1007/s11916-020-00877-5 · PubMed
- Fukui S, Ohseto K, Shiotani M. Patterns of pain induced by distending the thoracic zygapophyseal joints. Regional Anesthesia. 1997;22(4):332-6. doi:10.1016/s1098-7339(97)80007-7 · PubMed
- Dreyfuss P, Tibiletti C, Dreyer SJ. Thoracic zygapophyseal joint pain patterns. A study in normal volunteers. Spine. 1994;19(7):807-11. doi:10.1097/00007632-199404000-00014 · PubMed
- Slipman CW, Plastaras C, Patel R, et al. Provocative cervical discography symptom mapping. The Spine Journal. 2005;5(4):381-8. doi:10.1016/j.spinee.2004.11.012 · PubMed
- Kwanchuay P, Petchnumsin T, Yiemsiri P, et al. Efficacy and Safety of Single Botulinum Toxin Type A (Botox) Injection for Relief of Upper Trapezius Myofascial Trigger Point: A Randomized, Double-Blind, Placebo-Controlled Study. Journal of the Medical Association of Thailand. 2015;98(12):1231-6. PubMed
- Mehta LS, Beckie TM, DeVon HA, et al. Acute Myocardial Infarction in Women: A Scientific Statement From the American Heart Association. Circulation. 2016;133(9):916-47. doi:10.1161/CIR.0000000000000351 · PubMed
- Joshi SS, Hamra M, Newby DE. Diagnostic computed tomography in acute interscapular pain. Heart. 2020;106(2):126. doi:10.1136/heartjnl-2019-315821 · PubMed
Frequently Asked Questions
Most often it is musculoskeletal — myofascial trigger points and muscle overload in the rhomboids and mid-trapezius from desk posture, or referred pain from the joints of the thoracic spine. A frequently missed cause is the neck: the lower cervical discs and facet joints refer pain straight into the area between the shoulder blades, so an interscapular ache can actually be a neck problem. Less commonly the pain comes from a thoracic disc or shingles. A small number of cases are referred from internal organs (heart, aorta, gallbladder), which is why a few specific warning signs matter.
Go to an emergency room or call 911 if the pain is sudden and severe or feels like tearing or ripping (a possible aortic emergency), or if it comes with chest pressure, shortness of breath, sweating, nausea, lightheadedness, or pain spreading to the arm, neck, or jaw (a possible heart attack — and women, people with diabetes, and older adults can have less typical presentations). Also seek urgent care for upper-back pain with fever, unexplained weight loss, a history of cancer, or new leg weakness or loss of bladder or bowel control. These are uncommon, but they are the reasons not to simply assume every case is a muscle knot.
Yes, and it is one of the most overlooked causes. Provocative discography mapping shows the lower cervical discs — C3-C4 through C7-T1 — refer pain directly into the interscapular region. The same is true of the lower cervical facet joints. So a person with no neck pain at all can have a nagging ache between the shoulder blades that is actually generated in the neck. The practical clue is that the interscapular pain changes with neck position and is reproduced on neck examination, not by pressing the painful spot itself.
Sustained forward-head, rounded-shoulder posture loads the mid-trapezius and rhomboids and compresses the thoracic and lower cervical joints — and thoracic spine pain is consistently associated with office work, high workload, and prolonged sitting. The muscles between the shoulder blades work as postural stabilizers all day, develop trigger points, and ache by afternoon. Changing position, standing, and a posture-focused exercise program usually reduce it, which is itself a clue the cause is mechanical rather than internal.
For the common musculoskeletal causes, start with posture correction and targeted physical therapy for the deep neck flexors and scapular stabilizers. When myofascial trigger points are the driver, trigger point injections or botulinum toxin can help — a randomized trial found botulinum toxin raised the pressure-pain threshold in upper trapezius trigger points. When a thoracic facet joint is confirmed as the source, a medial branch block and then radiofrequency ablation give lasting relief. When the pain is referred from the neck, the treatment targets the cervical source. The first step is identifying which of these is actually generating the pain.
The most reliable way is a diagnostic block. If pressing and stretching the muscle reproduces the exact pain and a trigger point injection abolishes it, the muscle is the source. If the pain is reproduced by loading the thoracic facet joints or the neck and is relieved by a fluoroscopically guided medial branch block, the joint or the cervical spine is the source. Imaging alone does not settle it — degenerative changes look similar on MRI in painful and pain-free spines — so the block, not the scan, is the deciding test.
Most major commercial PPO plans cover an evaluation for interscapular and thoracic pain and the associated diagnostic injections, often with prior authorization. Modal Pain verifies your benefits before the first visit. We accept most major commercial PPO plans and do not participate with Medicare or Medicaid. <a href="/verify-insurance/">Check your plan</a> or call (646) 290-6660.


