Most people who end up with an occipital neuralgia diagnosis have spent months being treated for something else — tension headache, migraine, or “stress.” The pain sits at the back of the head, so it gets folded into the broad category of headache and managed with the medications that work for migraine. When those medications only blunt the edge and never stop the attacks, the reason is usually that the generator is a peripheral nerve, not the brain. The International Classification of Headache Disorders defines occipital neuralgia as a paroxysmal, shooting or stabbing pain in the distribution of the greater, lesser, or third occipital nerves, accompanied by tenderness over the involved nerve and eased, at least briefly, by a local anesthetic block [1].
What occipital neuralgia feels like
The pain is electric. Patients describe shocks, jabs, or a hot-poker sensation that starts where the neck meets the skull and shoots upward over the back and side of the head, sometimes reaching behind the eye on the same side. Attacks are brief but can repeat through the day. Between them, the scalp is frequently sore, numb, or hypersensitive — a quality clinicians call dysesthesia — and many patients can no longer tolerate a ponytail, a hat, or sleeping on the affected side [2].
It is usually one-sided, though it can affect both occipital nerves. A specific tender spot is common: pressing just below the bony ridge at the base of the skull, where the greater occipital nerve emerges, often reproduces the shooting pain and may send it racing up the scalp [2].
The nerves behind the pain
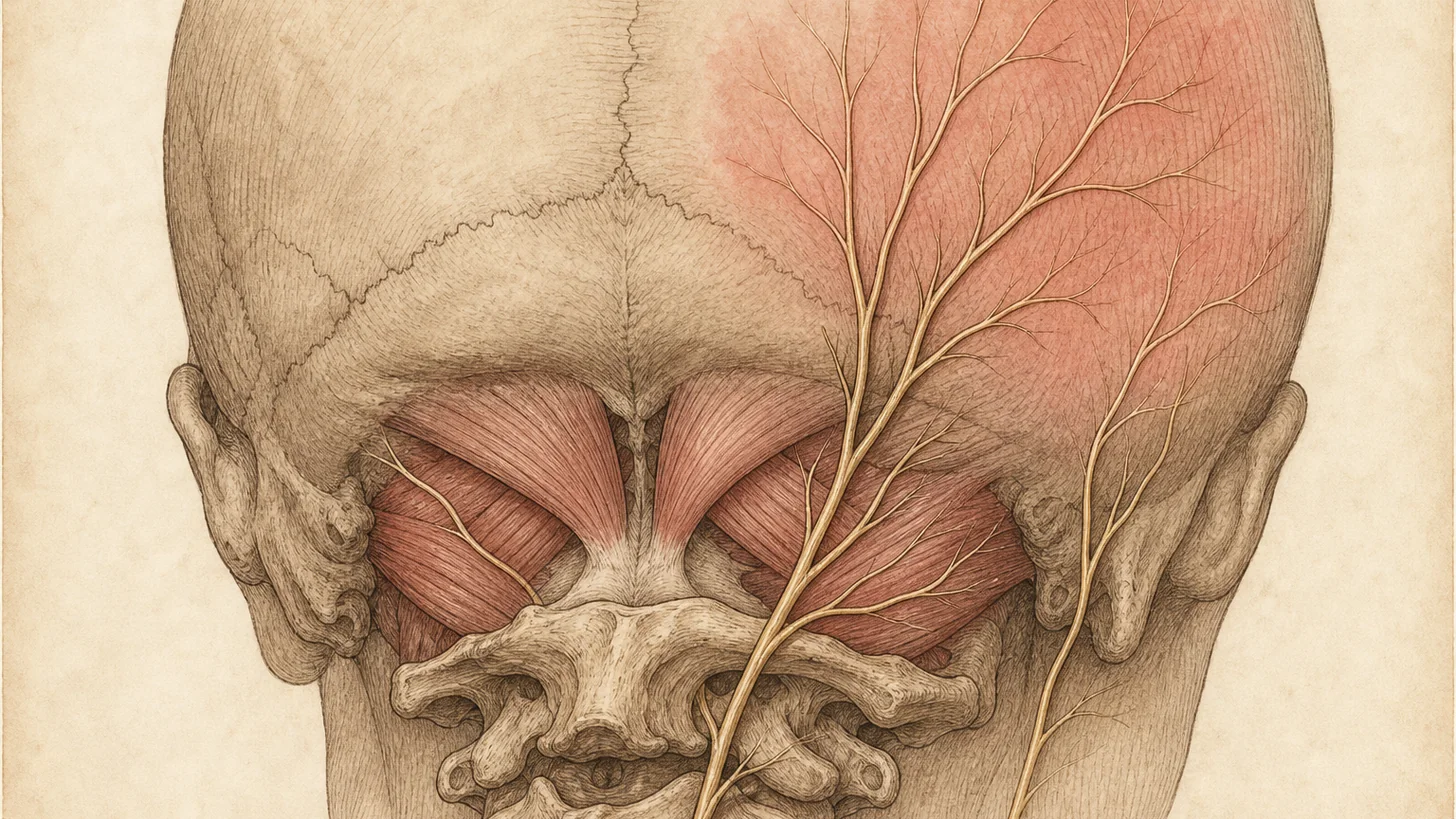
Three nerves carry occipital pain. The greater occipital nerve, the most commonly involved, arises from the C2 spinal nerve, curls around the suboccipital muscles, and supplies most of the back of the scalp. The lesser occipital nerve covers the area behind the ear, and the third occipital nerve, closely tied to the C2-C3 facet joint, covers the lower occiput [3]. Occipital neuralgia happens when one of these nerves is irritated, compressed, or inflamed along its course — by tight suboccipital muscles, by degenerative changes in the upper cervical spine, or in the aftermath of whiplash or a blow to the back of the head. In a large share of cases no single structural cause is found, and the condition is considered idiopathic [5][7].
Occipital neuralgia, migraine, and cervicogenic headache
Occipital pain has overlapping causes, and getting the label right changes the treatment. Migraine is a primary headache generated in the brain and its pain pathways — throbbing, often with nausea, light and sound sensitivity, and a response to triptans. Cervicogenic headache is referred pain from an upper cervical joint or disc, typically the C2-C3 facet, that travels to the head. Occipital neuralgia is pain arising from the occipital nerve itself. The three frequently coexist and share the same territory at the back of the head, which is why occipital neuralgia is so often misclassified [4].
One caution about the diagnostic block: numbing the occipital nerve relieves the pain of occipital neuralgia, but it can also relieve migraine and cervicogenic headache, so a positive response confirms the nerve as a pain conduit without proving the nerve is the sole source [5][6]. That is why the diagnosis is built from the whole picture — the shock-like quality, the nerve distribution, and the focal tenderness — and not from the block in isolation.
How occipital neuralgia is diagnosed
There is no blood test or scan that proves occipital neuralgia. Diagnosis follows the International Classification of Headache Disorders criteria: unilateral or bilateral paroxysmal shooting or stabbing pain in the occipital nerve distribution, tenderness over the affected nerve, and transient relief of the pain by a local anesthetic block of that nerve [1]. Imaging of the cervical spine has a role, but it is to exclude a secondary cause — a compressive lesion, inflammatory disease, or upper cervical pathology — rather than to make the diagnosis [2]. The anesthetic block is the closest thing to a confirmatory test, and because it doubles as a treatment, it is usually the pivot point between evaluation and management [6].
Evidence-based treatment
Because the pain comes from a peripheral nerve, effective treatment targets that nerve rather than masking head pain. The literature supports a stepped approach.
Conservative care comes first. Correcting the forward-head posture that loads the suboccipital muscles, targeted physical therapy to release those muscles, and nerve-stabilizing medication such as certain antiepileptics or tricyclic antidepressants are reasonable first steps for milder or recent-onset cases [4][2]. Our physical therapy program addresses the muscular component that often feeds the nerve irritation.
Occipital nerve block. When pain is severe or has not responded to conservative care, an occipital nerve block is the first-line minimally invasive step. Local anesthetic, often combined with a corticosteroid, is placed at the affected nerve. The block relieves pain in many patients and confirms the diagnosis at the same time, though the duration of relief from a single block can be short [6][2].
Botulinum toxin. For patients whose relief from blocks is incomplete or short-lived, an onabotulinumtoxinA injection is an option. The evidence suggests it tends to improve the sharp, shooting component of the pain more than the dull background ache [2]. We perform this as a targeted botulinum toxin injection, not a cosmetic dose.
Pulsed radiofrequency and radiofrequency ablation. When relief needs to outlast injections, pulsed radiofrequency applied to the occipital nerve can give longer-term control with minimal nerve destruction [6][7]. When the upper cervical facet joints are contributing — common given how closely the third occipital nerve is tied to the C2-C3 joint — a medial branch block confirms the joint as a target and radiofrequency ablation of that nerve can then provide months of relief, repeatable as the nerve regenerates [6].
Occipital nerve stimulation is reserved for refractory cases that have failed the steps above, placing a small lead near the occipital nerves to modulate the pain signal [6][2].
When to see a specialist
Brief electric shocks up the back of the head, a scalp too tender for a pillow, a focal sore spot at the base of the skull, or “migraines” that have never fully responded to migraine medication all warrant evaluation for occipital neuralgia. The sooner the nerve is confirmed as the source with a diagnostic block, the sooner targeted treatment can replace open-ended trials of the wrong medication.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. doi:10.1177/0333102417738202 · PubMed
- Pan W, Peng J, Elmofty D. Occipital Neuralgia. Current Pain and Headache Reports. 2021;25(9):61. doi:10.1007/s11916-021-00972-1 · PubMed
- Katta-Charles SD. Craniofacial neuralgias. NeuroRehabilitation. 2020;47(3):299-314. doi:10.3233/NRE-208004 · PubMed
- Barmherzig R, Kingston W. Occipital Neuralgia and Cervicogenic Headache: Diagnosis and Management. Current Neurology and Neuroscience Reports. 2019;19(5):20. doi:10.1007/s11910-019-0937-8 · PubMed
- Dougherty C. Occipital neuralgia. Current Pain and Headache Reports. 2014;18(5):411. doi:10.1007/s11916-014-0411-x · PubMed
- Lefel N, van Suijlekom H, Cohen SPC, Kallewaard JW, Van Zundert J. Cervicogenic headache and occipital neuralgia. Pain Practice. 2024;25(1):e13405. doi:10.1111/papr.13405 · PubMed
- Manolitsis N, Elahi F. Pulsed radiofrequency for occipital neuralgia. Pain Physician. 2014;17(6):E709-17. PubMed
Frequently Asked Questions
Sharp, electric, stabbing jolts that start at the base of the skull on one side and shoot up across the scalp toward the top of the head, often behind or above the ear. Between the jolts the scalp usually stays sore or tingling, and light touch — combing your hair, resting on a pillow, a shirt collar — can set off an attack. The pain follows the path of the greater, lesser, or third occipital nerve.
Occipital neuralgia is a shooting, shock-like nerve pain triggered by touch over a specific occipital nerve, and the scalp is tender between attacks. Migraine is a deep, throbbing, often whole-head pain with nausea and sensitivity to light and sound. The two can coexist, and a nerve block can relieve both, so diagnosis rests on the pattern of pain and the distribution of tenderness rather than the block alone.
By the International Classification of Headache Disorders criteria: paroxysmal shooting or stabbing pain in the distribution of the occipital nerves, tenderness over the affected nerve, and temporary relief of the pain by a local anesthetic block of that nerve. Imaging is used to rule out a structural cause in the upper neck rather than to confirm the diagnosis itself.
A stepped approach. Posture correction, physical therapy, and nerve-stabilizing medication come first. When pain is severe or persistent, an occipital nerve block is the first-line minimally invasive step and doubles as a diagnostic test. For relief that outlasts the block, options include botulinum toxin injection, pulsed radiofrequency of the occipital nerve, and — when the upper cervical facet joints contribute — radiofrequency ablation. Occipital nerve stimulation is reserved for refractory cases.
Some flares settle with rest, heat, and posture change, especially when a clear trigger like a long stretch at a screen or a minor neck injury is removed. When the pain is recurrent or constant, it tends not to resolve on its own, and a diagnostic occipital nerve block is the fastest way to confirm the source and start targeted treatment.