The description is consistent enough that it is almost diagnostic on its own: a band of burning pain that starts near the spine and wraps around one side of the chest or upper abdomen along the line of a rib, made worse by a deep breath or a twist, with a stripe of skin that hurts when a shirt brushes against it. Most people have had it explained as a pulled muscle, a pinched nerve, or — alarmingly — a possible heart problem. When it follows the path of a single rib and burns, the right name is intercostal neuralgia, and it is a nerve problem with a specific test and specific treatments.
Rule out the heart and lungs first
Chest-wall nerve pain is benign. The structures it can be confused with are not always. Before intercostal neuralgia is diagnosed, the dangerous causes of chest pain are excluded — that order is not negotiable.
Seek emergency care, not a clinic appointment, for crushing or pressure-like chest pain, chest pain with shortness of breath, sweating, nausea, or lightheadedness, pain spreading to the arm, neck, or jaw, or sudden breathlessness with sharp pain on breathing. Those can signal a heart attack, a pulmonary embolism, or other emergencies, and they are evaluated immediately. Intercostal neuralgia is the diagnosis that remains after the heart, lungs, and great vessels have been cleared — not a label to apply to undiagnosed chest pain.
What intercostal neuralgia actually is
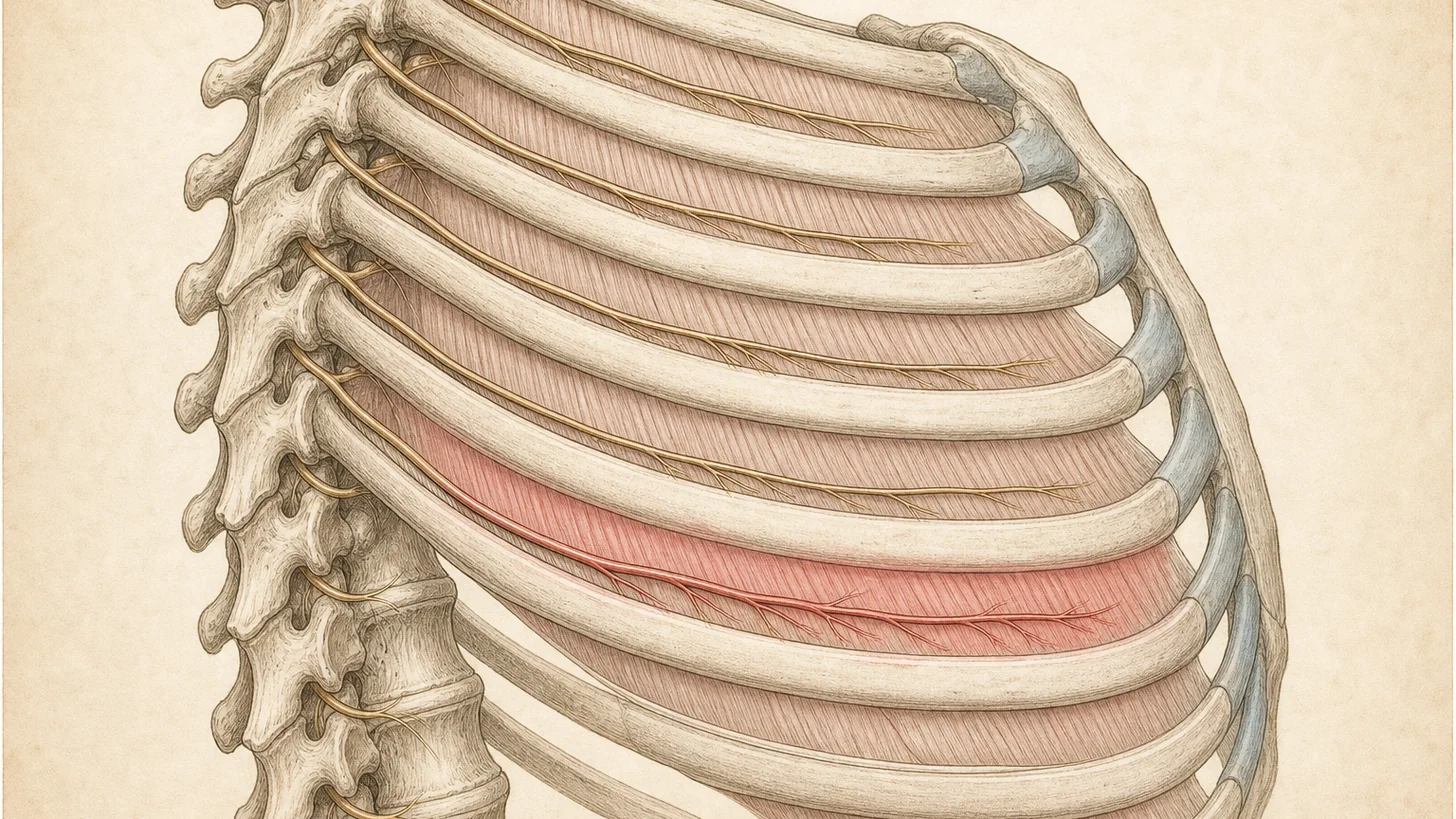
Each intercostal nerve is the continuation of a thoracic spinal nerve. It runs forward in the costal groove along the underside of its rib, accompanied by the intercostal artery and vein, and supplies the muscles and skin of the chest and upper-abdominal wall in a narrow band. There are eleven pairs, and the band each one serves wraps around the trunk like a hoop. Intercostal neuralgia is neuropathic pain in that distribution — pain generated by the nerve itself rather than by the muscle, joint, or cartilage nearby [1]. That is why it burns and shoots rather than aches, and why the overlying skin is often hypersensitive.
This also explains the differential. A pulled intercostal muscle is a dull mechanical ache that hurts with movement but does not burn. Costochondritis is tenderness directly over the rib-cartilage junctions beside the breastbone, reproduced by pressing there. Two close relatives are pain from the terminal branches of these same nerves: intercostobrachial neuralgia after breast surgery, which is felt in the armpit and inner arm, and anterior cutaneous nerve entrapment (ACNES), which is felt as a focal spot on the abdominal wall. Intercostal neuralgia proper is the band along the rib itself.
What causes it
Chest surgery is the leading cause. Chronic pain after thoracotomy affects roughly a quarter to more than half of patients, and a critical review of the mechanisms concluded that intercostal nerve injury is the single most important pathogenic factor [2]. Breast surgery, rib surgery, and chest-tube placement can injure these nerves the same way. Notably, deliberately cutting the nerve is not a reliable fix: a randomized trial of intercostal neurectomy during thoracotomy did not reduce the rate of chronic post-thoracotomy pain [3]. The lesson is that these nerves are better managed than severed.
Shingles is the classic non-surgical cause. Herpes zoster reactivates along a dermatome, and the thoracic dermatomes are the most commonly affected region [4]. The acute rash can be followed by post-herpetic neuralgia — a burning, band-like pain along the same rib that can persist for months. Treating the nerve early matters here, because it changes the odds of that lasting pain.
Trauma and entrapment. Rib fractures, blunt chest trauma, and even forceful coughing can injure or irritate an intercostal nerve, producing a post-traumatic neuralgia along the affected space [7]. Some cases have no clear trigger at all, with the nerve entrapped or irritated as it courses through the chest-wall muscles.
How it’s diagnosed
After the heart and lungs are cleared, the diagnosis is clinical and confirmed by a block. The history is usually distinctive — a band of burning pain along one rib, often after surgery, shingles, or trauma. The examination maps the pain to a single intercostal level and looks for allodynia along that band. Imaging is used to find a cause (a rib fracture, post-surgical change) or to exclude something else, not to make the diagnosis, because a nerve this small is not what a routine scan shows.
The decisive test is an image-guided intercostal nerve block. A small volume of local anesthetic is placed at the costal groove of the suspected nerve under ultrasound or fluoroscopic guidance — both more accurate than a blind landmark technique [1]. If the familiar band of pain goes quiet in the anesthetic window, the nerve is confirmed as the generator, and the block doubles as the first treatment.
Evidence-based treatment
Treatment is stepped, and most of it is in the interventional pain wheelhouse.
Neuropathic-pain medication first. Gabapentin or pregabalin, and topical agents such as a lidocaine patch over the band, are the reasonable starting point for the nerve pain itself.
Image-guided intercostal nerve block. This is the workhorse — diagnostic and therapeutic in one step, repeatable, and more accurate and safer under ultrasound or fluoroscopy than a landmark approach [1]. With a corticosteroid added, relief can last weeks to months.
Early blocks when shingles is the cause. In acute herpes zoster, an ultrasound-guided intercostal nerve block has been shown to reduce the acute pain burden and lower the incidence of lasting post-herpetic neuralgia — so treating the nerve early is not just about comfort, it changes the trajectory [5].
Radiofrequency ablation for refractory cases. When the pain keeps returning after positive diagnostic blocks, radiofrequency ablation of the intercostal nerve can provide durable relief — in reported cases, well beyond a year [6]. Regional plane blocks (such as a serratus anterior plane block) are a further option for post-surgical and post-traumatic chest-wall pain [7].
Surgery to cut the nerve is generally not the answer — as the neurectomy trial showed, severing the intercostal nerve does not reliably prevent or relieve the pain [3]. The durable wins come from calming and modulating the nerve, not removing it.
When to see a specialist
Once the heart and lungs have been cleared, see an interventional pain physician if a burning, band-like rib pain has lasted more than a few weeks, has followed chest or breast surgery, has lingered after a bout of shingles, or has not responded to neuropathic-pain medication. The diagnostic intercostal nerve block answers the question and starts the treatment in the same visit. And do not sit on the emergency features above — chest pain with pressure, breathlessness, or radiation to the arm or jaw belongs in an emergency room.
Verify your insurance covers an intercostal neuralgia workup Book a same-week diagnostic block
Or call (646) 290-6660.
For the broader framework on peripheral nerve pain, see the peripheral nerve entrapment page; for chest-wall nerve pain after breast surgery specifically, see post-mastectomy nerve pain.
References
This article is reviewed against the peer-reviewed literature. Citations retrieved from PubMed.
- Elkhashab Y, Wang D. A Review of Techniques of Intercostal Nerve Blocks. Current Pain and Headache Reports. 2021;25(10):67. doi:10.1007/s11916-021-00975-y · PubMed
- Wildgaard K, Ravn J, Kehlet H. Chronic post-thoracotomy pain: a critical review of pathogenic mechanisms and strategies for prevention. European Journal of Cardio-Thoracic Surgery. 2009;36(1):170-80. doi:10.1016/j.ejcts.2009.02.005 · PubMed
- Koryllos A, Althaus A, Poels M, et al. Impact of intercostal paravertebral neurectomy on post thoracotomy pain syndrome after thoracotomy in lung cancer patients: a randomized controlled trial. Journal of Thoracic Disease. 2016;8(9):2427-33. doi:10.21037/jtd.2016.07.93 · PubMed
- Shiraki K, Toyama N, Shiraki A, Yajima M. Age-dependent trigeminal and female-specific lumbosacral increase in herpes zoster distribution in the elderly. Journal of Dermatological Science. 2018;90(2):166-71. doi:10.1016/j.jdermsci.2018.01.009 · PubMed
- Xue M, Yuan R, Yang Y, Qin Z, Fu R. Application of ultrasound-guided thoracic paravertebral block or intercostal nerve block for acute herpes zoster and prevention of post-herpetic neuralgia: A case-control retrospective trial. Scandinavian Journal of Pain. 2024;24(1). doi:10.1515/sjpain-2024-0030 · PubMed
- Abd-Elsayed A, Lee S, Jackson M. Radiofrequency Ablation for Treating Resistant Intercostal Neuralgia. The Ochsner Journal. 2018;18(1):91-93. PubMed
- Sir E, Eksert S, Ince ME, et al. A Novel Technique: Ultrasound-Guided Serratus Anterior Plane Block for the Treatment of Posttraumatic Intercostal Neuralgia. American Journal of Physical Medicine & Rehabilitation. 2019;98(11):e132-e135. doi:10.1097/PHM.0000000000001121 · PubMed
Frequently Asked Questions
Intercostal neuralgia is neuropathic pain in the distribution of an intercostal nerve — the nerves that run in the groove under each rib and supply the chest and upper-abdominal wall. The pain is typically a burning, stabbing, or electric band that follows one rib space and wraps from the back around toward the front of the chest or abdomen, often with skin that is hypersensitive to light touch. It is a nerve problem, not a muscle or cartilage problem, which is why it does not behave like a simple strain.
A band of burning, stabbing, or shooting pain along one rib, usually on one side, that can wrap from the spine around to the front. It is often made worse by deep breathing, coughing, laughing, twisting, or reaching, and the overlying skin can be painfully sensitive to clothing or a light touch (allodynia). Because the pain moves with breathing and is in the chest, it is frequently mistaken at first for something in the heart or lungs — which is exactly why those have to be ruled out before the nerve is blamed.
The common causes are surgery, shingles, and trauma. Chest surgery is the biggest: chronic pain follows thoracotomy in roughly a quarter to more than half of patients, and intercostal nerve injury is considered the chief mechanism. Breast and other chest-wall surgery can do the same. Shingles (herpes zoster) most often strikes the thoracic dermatomes, and can leave lasting post-herpetic neuralgia along a rib. Rib fractures and chest trauma are another common trigger, and some cases are idiopathic — the nerve is irritated or entrapped without a clear inciting event.
A heart attack or other cardiac and lung emergencies are ruled out first — crushing chest pressure, shortness of breath, sweating, or pain radiating to the arm or jaw needs emergency care, not a clinic visit. Once those are excluded, the difference from musculoskeletal causes is the quality and pattern. A pulled intercostal muscle is a dull, mechanical ache that hurts on movement but is not burning or electric. Costochondritis is tenderness right over the rib-cartilage junctions near the breastbone, reproduced by pressing there. Intercostal neuralgia is neuropathic — burning, band-like, following the nerve, with skin hypersensitivity — and it is confirmed by an intercostal nerve block that abolishes the pain.
Treatment is stepped. Neuropathic-pain medications (such as gabapentin or pregabalin) and topical agents come first. The workhorse is an image-guided intercostal nerve block, which is both the diagnostic test and a therapeutic treatment; ultrasound or fluoroscopic guidance is more accurate than a landmark-based technique. When shingles is the cause, an early intercostal nerve block can reduce the acute pain and the risk of lasting post-herpetic neuralgia. For pain that keeps returning after positive blocks, radiofrequency ablation of the nerve can give durable relief, and regional plane blocks help post-surgical and post-traumatic cases.
Yes, and it does two jobs at once. Numbing the suspected intercostal nerve with local anesthetic both confirms the diagnosis — if it abolishes your familiar band of pain, the nerve is the source — and provides therapeutic relief, especially when a corticosteroid is added. Image guidance with ultrasound or fluoroscopy improves accuracy and lowers the (low) risk of complications compared with a blind landmark technique. The block is repeatable, and it tells us whether a longer-lasting treatment like radiofrequency ablation is likely to help.
Most major commercial PPO plans cover an evaluation for intercostal neuralgia and image-guided intercostal nerve blocks, often with prior authorization. Modal Pain verifies your benefits before the first visit. We accept most major commercial PPO plans and do not participate with Medicare or Medicaid. <a href="/verify-insurance/">Check your plan</a> or call (646) 290-6660.


